Key in the fight against the pandemic, the SUS is facing funding and governance issues, both old and new
Patient landing in Lagoa-Barra field hospital, in Rio de Janeiro, set up at the start of the pandemic
Allan Carvalho / AGIF / AFP
The pandemic has killed more than 220,000 people in Brazil and has caused overcrowding in emergency rooms (ERs) and intensive care units (ICUs). It has also exposed both the importance and the weaknesses of the Sistema Único de Saúde (Unified Health System – SUS), which provides free and universal healthcare to the population, especially the 150 million Brazilians (71.5%) who have no private health insurance. Thanks to its decentralized structure in states and municipalities, nearly 100 field hospitals were built, 3,100 extra ICU beds were made available in public hospitals, health surveillance teams have begun monitoring social distancing, and 3,300 teams of the Emergency Medical Mobile Service (SAMU) are available to respond to emergencies and to transport patients. In 2021, the challenge lies in vaccinating the population against the novel coronavirus—the SUS has 37,600 vaccination rooms all over the country.
However, the flaws with SUS have also been made clearer by this healthcare emergency. Persistent inequality in access to healthcare, limited funding, and management issues have been illustrated by the collapse of the system in Manaus and its inability to provide mass testing. “Despite everything, the SUS was a gift during the pandemic,” says public health officer Reinaldo Guimarães, a professor at the Federal University of Rio de Janeiro (UFRJ) and vice president of the Brazilian Association of Collective Health (ABRASCO). “Without it, our situation would have been much worse—as seen in countries where people cannot seek care because they cannot afford it.”
An October report by a group of experts from ABRASCO assessed how the SUS performed and pointed out that the system has yet to become fully consolidated. The document lists its achievements and some of the goals it has yet to meet. On the one hand, there has been a drop in infant mortality and increased life expectancy, as well as successful vaccination, battling AIDS, and organ transplant programs. On the other hand, there is still a high prevalence of tuberculosis and leprosy, as well as neonatal syphilis, and excessive cesarean section deliveries. “Services and coverage have been expanded, particularly in primary care, but access to specialized services is still limited and there is a lack of communication between care facilities,” he concludes. Experts have proposed measures to improve the SUS. They mainly involve ensuring regular and sufficient funding and further investing in primary care, by expanding the scope of programs such as the Family Healthcare Strategy to reduce healthcare gaps in the country.
The SUS was implemented through the 1988 Constitution, which says healthcare “is a universal right and a duty of the State, provided through social and economic policies aimed at reducing the risk of disease and other health problems, and ensuring universal and equal access to actions and services for the promotion, protection, and recovery of health.” Its implementation depended on a set of public policies based on coordinated and solidary action from federal, state, and local governments for primary and specialized care, health and epidemiological surveillance, and pharmaceutical care.
“From 1994 to 2002, the SUS underwent many updates, such as the requirement of more funding from state and local governments, and the provision of federal funds to implement specific programs,” explains healthcare economist André Medici, who worked at the World Bank and at the Inter-American Development Bank. During the following period, says Medici, some of that momentum was lost. “There have been innovations, such as the national tobacco control program, but the system now operates under a more political logic, emphasizing the allocation of funds to states and municipalities—which made room for the siphoning of funds, such as the 2006 “Ambulance Mafia” (a corruption scandal involving the diversion of funds meant for the purchase of ambulances). In recent years, the system has been dealing with an ever-worsening economic situation, and a population that has become increasingly unable to afford private health insurance.”
Before the SUS, only the Brazilians who made regular social security payments were covered by the public healthcare system, while the poor and unemployed depended on charity hospitals. Inspired by the’s National Health Service of the United Kingdom (UK), the SUS was established with great ambitions. No other public healthcare system in the world claims to treat such a large population without imposing restrictions or copay mechanisms. “I have no knowledge of any universal healthcare system in the world handling such a large territory, population size, and regional and social inequalities of Brazil with the level of performance and achievements that the SUS has had in just 30 years, despite its many challenges,” says Jairnilson Silva Paim, professor at the Federal University of Bahia. “I am often reminded of the Italian National Health Service which, like the SUS, has suffered a type of ‘character assassination.’ Despite Italy’s long history and culture, it took 30 years—from 1948 to 1978—to transform the constitutional principle of the right to healthcare into law. Brazil, on the other hand, was able to do this in two years, first passing the regular healthcare bill and then the SUS bill.”
Patients seeking care in the clinics of the Clinics Hospital of São Paulo, the largest hospital complex in Latin AmericaLéo Ramos Chaves
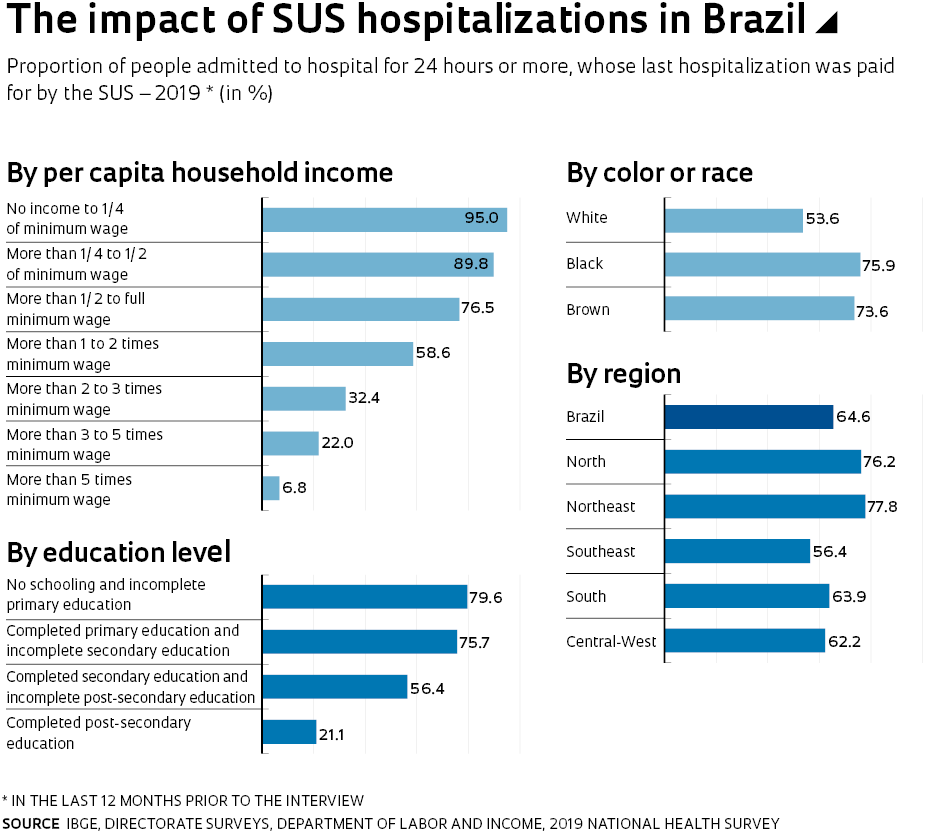
The chasm between the great aspirations of the SUS and its funding helps explain why so many of its goals have not been achieved. The idea of making it accessible to all has never materialized. The SUS became known as a resource for the poor, while the middle and upper classes resorted to private insurance plans and specialized care to ensure higher quality or faster access. According to the National Health Survey of the Brazilian Institute of Geography and Statistics (IBGE), 28.5% of the Brazilian population had access to private health insurance in 2019, compared to just over 5% in the 1980s. Private health insurance is more expensive than public healthcare in Brazil. The government healthcare expenses are equivalent to 3.9% of the gross domestic product (GDP), while private healthcare costs families 5.4% of the GDP.
Brazil spends much less on healthcare than countries that boast universal systems. According to data gathered by Fabiola Sulpino Vieira, public policy expert from the Institute of Applied Economic Research (IPEA), published last year in an article in Revista de Saúde Pública (Journal of public health), Brazil’s public healthcare spending per capita was US$606 in 2017. In Turkey, it was US$921; in the UK, it was US$3,300; in Germany, it was US$4,900. These were corrected according to each country’s purchasing power. According to the article, between 2014 and 2018, per capita expenditures dropped 2% for the federal government, 5% for state governments, and 2% for municipal governments.
Field hospital in Santo André, in the São Paulo metropolitan areaGustavo Basso / Nurphoto / Nurphoto Via AFP
Over its three decades of existence, the SUS has faced several funding issues. “The system was never seen as a priority when allocating public funds and has always had to fight for resources,” says Vieira. In the 1990s, a provisional tax was placed on financial transactions, the CPMF, as a campaign by then Minister Adib Jatene (1929–2014) to add funding for the SUS. Despite the law determining that funding must be allocated to healthcare, the ministry budget has not been increased and, in 1999, the CPMF earnings went to poverty eradication programs and efforts to reduce the pension deficit. It was abolished in 2007. A milestone for the consolidation of the SUS was the 29th Constitutional Amendment in 2000, which set a minimum percentage for federal, state, and municipal earnings to be allocated to the SUS budget.
In recent years, its funding has been threatened by restrictions imposed by the 95th amendment in 2016, which froze government spending for 20 years. In 2018 and 2019, the Ministry of Health budget was merely adjusted for inflation. In 2020, it may be exceeded because of emergency spending due to the pandemic. But the 2021 spending bill, passed last December, reinforced the budget ceiling and stipulated the health budget at R$134 billion—approximately R$30 billion less than last year. A public petition with 583,000 signatures was delivered to Congress by the National Health Council, asking that the ministry’s 2021 budget be at least R$168.7 billion. Some of the reasons for that include the ongoing pandemic, plus surgeries and appointments that have been postponed from 2020, which should drive up demand for medical services in 2021.
An application developed by the Ministry of Health—the Coronavirus SUS—with useful information about the diseaseLéo Ramos Chaves
The SUS is likely to get extra funding. An interim measure presented last December opened a R$20 billion credit for the purchase of vaccines. In practice, nothing prevents the government and Congress from increasing the health budget, if funding is moved from other areas and the overall expenditure ceiling is maintained. However, the logic for budget approval has been to freeze spending in a linear manner. One of the natural implications of this is a drop in per capita spending. “The Brazilian population grows 0.8% every year, and available funding should grow at least at the same rate,” states economist and expert on SUS funding Francisco Rózsa Funcia, from the University of São Caetano do Sul. “The elderly population, who have a higher incidence of chronic diseases, grows by 3.8% every year, which also increases costs to the system.”
Since the budget ceiling will be in place until 2036, another SUS issue is expected to worsen: governance. With lower funding, the federal government will have progressively less capacity to promote public health policies. It was the Ministry of Health who proposed innovative programs, such as the Family Healthcare Strategy or SAMU, pledging to provide funding for municipalities to maintain them. As an example, Vieira, from IPEA, mentions average and high complexity services, which require qualification by the Ministry of Health to be provided in municipalities. “To increase the number of beds for cancer patients, a state or municipal hospital needs federal authorization. Today, the ministry tends to be conservative in giving out these authorizations, because if it does, it will be obliged to provide funding for these beds and is impeded from further spending,” explains the researcher.
In another study published last December in the journal Saúde em Debate (Health in debate), Vieira and her IPEA colleague Luciana Servo showed how the Ministry of Health has been reducing its role as system coordinator. According to the study, the share of the SUS budget that is not controlled by the Ministry, and which is linked to parliamentary amendments, has increased: from R$240 million, in 2014, to R$6.6 billion, in 2018. This issue has worsened during the pandemic, not due to budget challenges, but to the different ways federal, state, and municipal governments have approached the health emergency. The SUS was partly managed by the National Council of Health Secretariats (CONASS). The article lists occurrences that “illustrate the escalating conflict in the tripartite relationship” as a factor that kept representatives from state and municipal health secretariat councils from attending the inauguration of Health Minister Nelson Teich, in April, and the “carelessness on the part of these councils in the decision making regarding pandemic efforts, such as publishing material on the use of chloroquine and hydroxychloroquine to treat COVID-19, without submitting it for analysis by the National Commission for the Incorporation of Health Technologies.”
If there is one improvement to the SUS that all sides agree on, it is the need for further investment in primary care—the gateway to the system, which provides simpler care and forwards more complex cases to expert services. Primary care programs for the SUS have produced remarkable results, such as the Family Healthcare Strategy. Launched in 1994, the program is decentralized, with funds from both federal and municipal governments and makes essential care available to marginalized and remote populations. The program has grown over the past 20 years and today boasts more than 43,000 teams, made up of general practitioners, nurses, dentists, technical assistants, and community health workers, covering nearly all Brazilian municipalities. A study published in 2020 mapped the impact of the program in reducing infant mortality by analyzing the results of more than 50 scientific papers on the subject. From 1994 to 2017, the rate of children who died in their first year fell from 43 per 1,000 live births to 12.4 per 1,000 live births. The paper, coordinated by economist Naercio Menezes of the INSPER Education and Research Institute, noted that the drop was most significant in the municipalities covered by the program: after eight years, the rate of infant deaths dropped from 20% to 34%.
There are also economic reasons to invest more in primary care. Many of the SUS expenses are related to hospital stays. A 2018 assessment by the World Bank indicated inefficiencies in the use of funding that, once corrected, could save 23% in primary care expenditures and up to 34% in secondary and tertiary care. “The SUS is not the only healthcare system in the world that has inefficiencies; other countries do as well,” says André Medici. “The SUS is still ‘hospital-focused’ and needs to be better organized to treat patients. People are not used to going to clinics or healthcare centers. They go straight to the hospital. Once there, there are two possible outcomes: either the hospital cannot afford to treat them, or, if it can, the patient gets admitted for a few days, costing the system R$3,000 to R$4,000 per day—a much higher cost than if that same service had been provided at a primary care center. In many cases, the issue could be resolved by a family doctor.” Medici believes fixing these problems is key. “Managing available funding in a rational manner is important—even when the ultimate goal is to expand the system.”
Fabiola Vieira believes inefficiencies must be solved. “Unfortunately, many studies on the efficiency of the system end up commissioned and then used to justify budget cuts instead of signaling the need for measures to improve its performance,” she laments. Dr. Ligia Giovanella, a researcher at the Oswaldo Cruz Foundation National School of Public Health (ENSP-FIOCRUZ) warns that identifying inefficiencies in primary care ignores factors such as the geographical, economic, and social development of municipalities. “It is inappropriate to suggest budget cuts to a system as underfunded as the SUS.”
A major challenge to improve primary care is organizing care in regionalized networks. Most municipalities in Brazil have a small population and lack the funds and management capacity. The original design of the SUS provided for the establishment of these networks, but only in 2011 did the government divide the country into 430 healthcare regions, each covering 500,000 to 600,000 people. The goal is coordinating actions without overlapping efforts, ensuring access to primary and specialized care for all. The development of these networks has been uneven. “In some states, such as Ceará, state and municipal governments have partnered to offer clinics and specialty dental care centers in each region. The state of São Paulo has well-established regional structures, but in other places, coordination is challenging,” explains Giovanella. The researcher says that Municipal Health Secretariats meet in regional intergovernmental commissions to organize the actions of the networks, but dilemmas often arise. “There are no regional governments. Healthcare actions are the responsibility of municipal governments,” she states.
Family Health Team treating a woman in Marabá, Pará Paulo Sérgio Dos Santos – Marabá City Hall, Pará
She goes on to explain that coverage by family health teams should become universal, increasing it from the current 63% to at least 90% of the population. “Primary care, when well structured, can solve over 80% of health needs, but it should not be detached from a quality care network,” she says. Giovanella believes one of the barriers to improve primary care is the lack of family physicians. “In medical schools, few students are interested in general medicine.”
Apart from reorganization measures, expanding the scope of healthcare in Brazil will depend on the country’s capacity and willingness to invest more in public health policies. A May 2020 report from the Federal Court of Accounts (TCU) estimated that the SUS needs R$31 billion to fix its current shortcomings. These funds would need to be invested in family health teams, dental care, medical consultations and hospitalizations, tests, and hemodialysis sessions, which are currently underfunded. The document states that tension generated by the needs of the population and the limited funding available will likely increase. “On the one hand, the need for funding for the SUS is increasing, while the fiscal scenario seems unfavorable to increased spending.”
In a paper published in the journal Ciência & Saúde Coletiva (Science & collective health), economist Francisco Funcia came up with options to extend the funding for the SUS, such as allocating a fraction of the funding currently assigned to the public debt or reducing tax waivers for private healthcare expenses. In one of his projections, Funcia calculated how much additional funding the SUS would have today if the 2013 bill Saúde+10 had not been rejected by Congress. It proposed that a minimum of 10% of the country’s gross revenues be invested in healthcare. The additional amount, estimated at R$36 billion in 2018, would have been enough to quadruple the funding for the Basic Care Minimum given to municipalities, the amount invested in the supply of medications, and the SAMU spending, while also increasing by 50% funding for the Family Healthcare Strategy. “These data show that it is fiscally possible to pursue a political equation that results in additional federal funding for the SUS in the short term without the need for a tax reform and without compromising the balance of public accounts,” states Funcia.
Improving the SUS through science Program encourages researchers to solve problems in the healthcare system
The production of knowledge to improve the Unified Health System (SUS) has inspired thousands of Brazilian scientists through the SUS Research Program (PPSUS). The initiative, which has sponsored 172 public requests for proposals (RFPs) in 27 states, has invested R$395 million in nearly 4,000 projects since 2002. It is funded by the Ministry of Health through its Department of Science and Technology (DECIT), partnered with state health departments and research foundations.
The goal of PPSUS is to encourage researchers to solve SUS challenges in their area. “We work with the state health departments to identify the key management and care issues faced by the SUS locally and how academia can help mitigate them,” explains Marge Tenório, national coordinator of the program of the Ministry of Health. She highlights the role of PPSUS in the development of human resources specialized in healthcare: among employees and scholarship beneficiaries, 500 scientists obtained their master’s degrees, and 300 obtained their PhD through projects funded by the program.
Impactful projects are being developed in all regions of the country. Daniel Canavese, from the University of Rio Grande do Sul, helped improve the health surveillance of vulnerable populations by assessing situations of violence in the state according to race, gender, and sexual orientation. Thais Gigonzac, from the State University of Goiás, created strategies for genetic research and early intervention for individuals with autism spectrum disorder in the local healthcare system. Isabella Monlléo, from the Federal University of Alagoas, developed a strategy to create a referral system for the care of cleft palate patients.
Since 2006, in collaboration with the Ministry of Health, FAPESP has supported 241 projects of researchers from São Paulo institutions through PPSUS RFPs. “Our goal is that the results of the projects be incorporated into services and the healthcare system. Some projects are more applied, while others test new technologies. While some appear to have a smaller scope, their impact is often felt later,” says Maritsa Bortoli, researcher at the Health Institute of São Paulo, who has been a national coordinator for PPSUS and now works with the program at the Secretariat of Health of São Paulo. One of the top projects was led by ophthalmologist Antonio Carlos Lottelli Rodrigues, from São Paulo State University (UNESP) School of Medicine of Botucatu. It focuses on developing a line of care for children with abnormal results in the traditional eye test, which has been implemented throughout the state of São Paulo. While the test is mandatory for newborns in São Paulo, the diagnosis did not prevent many children with congenital cataracts from suffering long-term consequences of the condition due to delayed treatment. Congenital cataracts affect one in 2,500 newborns and, unless they are surgically corrected before the child is three months old, they can cause permanent blindness. “Parents would often get a diagnosis but could not have the surgery done through the SUS in time,” shares the researcher.
Supported by the Secretariat of Health of São Paulo and researchers from the medical schools of the University of Campinas (UNICAMP), University of São Paulo (USP), Federal University of São Paulo (UNIFESP), and Santa Casa of São Paulo, Lottelli developed a workflow that speeds up treatment. Now, whenever a hospital detects a suspected case of a congenital cataract, a test is scheduled to confirm the diagnosis at a clinic near where the family lives. If confirmed, the case is immediately referred to one of the six university hospitals associated with the project, where the surgery is performed. In Botucatu alone, the service directed by Lottelli has performed over 200 surgeries scheduled through this line of care.
There are also projects focused on improving the management of the SUS. An initiative coordinated by Cinira Fortuna, from the USP School of Nursing in Ribeirão Preto, helped transform the practices of professionals tasked with developing national policies for the humanization of care, management of the SUS, and permanent health education, in 24 municipalities covered by the Regional Health Department of Araraquara, São Paulo. These professionals, who help organize and support the implementation of these policies, are assessed by the Center for Development and Qualification for the SUS (CDQ-SUS) from the Araraquara region, since they work alongside healthcare staff in the municipalities.
The project brought together about 40 professionals for workshops and group discussions, encouraging them to think through and discuss the challenges they are facing. As a result, a “toolbox” was put together, containing shared practices and solutions that can help address communication problems with healthcare staff. “These professionals are essential for regional communication of policies, but they lacked the support to respond to challenges,” explains Fortuna, who implemented the project alongside Monica Vilchez and Ana Franceschini, from the Araraquara CDQ-SUS.
Reinaldo Guimarães, UFRJ researcher who was Secretary of Science, Technology and Strategic Inputs with the Ministry of Health from 2007 to 2010, points out that, in this century, those responsible for managing the healthcare system in Brazil have come to play a greater role in defining research policy—and the establishment of PPSUS and DECIT, with funding for basic and applied science, is an example of this. “In countries like the United States, Canada, and the UK, agencies that specifically fund healthcare research have been established,” he says. “Over the past 50 years, the concept of healthcare research has been expanded to include areas such as biochemistry and microbiology, which have begun to generate technologies and innovations that affect the population’s quality of life.”
The SUS-related projects funded by FAPESP can be found at bit.ly/2XPieIL.
This article may be republished online under the CC-BY-NC-ND Creative Commons license. The Pesquisa FAPESP Digital Content Republishing Policy, specified here, must be followed. In summary, the text must not be edited and the author(s) and source (Pesquisa FAPESP) must be credited. Using the HTML button will ensure that these standards are followed. If reproducing only the text, please consult the Digital Republishing Policy.