Psychiatric problems may be the first signs of Alzheimer’s disease
Sample of cerebral areas associated with memory, affected by microscopic lesions typical of Alzheimer’s (brown section)
Léo Ramos Chaves
Difficulty finding the car keys, which were absentmindedly placed in the sock drawer instead of the usual key holder, or the terrifying inability to remember the way home after going for a run through the neighborhood, as experienced by the university professor in the 2014 movie Still Alice, may not be the first signs of Alzheimer’s disease. The illness, which was identified slightly more than a century ago by German psychiatrist and neuroanatomist Alois Alzheimer and almost simultaneously by Czech psychiatrist and neuroanatomist Oskar Fischer, gradually destroys brain cells and is known for erasing memory and reducing the ability to plan and carry out daily tasks, such as writing a grocery list. These signs, however, are typical of the advanced stages of the disease. Much earlier, it can manifest in a more disguised manner, being confused with more common societal problems, such as depression, anxiety, or abrupt changes in sleep patterns or appetite.
For some time, it has been known that these psychiatric disturbances are more frequent among people who develop Alzheimer’s as they age than among the healthy senior population. Based on population studies, some neurologists and mental health experts argue that depression and anxiety appear first, caused by isolation and other difficulties one faces with aging, and, if left untreated, increase the risk of Alzheimer’s. Evidence is beginning to appear that, at least in some cases, the opposite may occur: these psychiatric events result from neurological lesions in the initial stages of Alzheimer’s disease.
There are solid indications from the work of Brazilian neuropathologist Lea Tenenholz Grinberg that psychiatric problems precede memory loss and dementia, which arise two to three decades after the first neurological damage of Alzheimer’s. Tenenholz Grinberg, a professor at the University of São Paulo (USP) and the University of California in San Francisco (UCSF) in the United States, along with her Brazilian and North American colleagues, observed that after the first lesions appear the risk of psychiatric problems increases. The probability of developing anxiety and changes (increases or decreases) in appetite and sleep is three times greater for those with the initial lesions than for those without. Furthermore, the risk of depression and of restlessness are four times and six times greater, respectively. “These results indicate that, in some cases, Alzheimer’s already exists in areas that modulate cerebral activity when the first psychiatric events appear,” confirms Tenenholz Grinberg.
Specimens of brain tissue stored at the Biobank for the Study of Aging at USPLéo Ramos Chaves
Researchers arrived at this conclusion after analyzing the brains of 455 people between the ages of 58 and 82. The brain specimens had been stored in the Biobank for the Study of Aging at USP, one of the largest brain collections in the world. This collection holds 3,000 specimens that have been donated by the families of individuals who had been autopsied by the Capital’s Death Verification Service in São Paulo. In the study, the authors did not analyze only the brain. They also inspected the brainstem, which, together with the cerebellum and the brain, comprise the encephalon, a group of structures housed in the skull. In 2009, Tenenholz Grinberg and the teams of the German neuroanatomist Helmut Heinsen, at the time with the University of Würzburg in Germany, and the teams of neurologist Ricardo Nitrini and geriatric physician Wilson Jacob Filho, both from USP, confirmed that one of the first structures damaged by Alzheimer’s was the brainstem and not the brain.
More recently, in an article published in October 2018 in the Journal of Alzheimer’s Disease, the researchers grouped the cases according to the classification proposed by the German neuroanatomists Heiko Braak and Eva Braak (1939–2000). Presented in 1991, the scale organizes cases of Alzheimer’s in six stages, which increase in severity as the number of lesions and affected areas of the encephalon grows. The scale was revised in 2011 by Heiko Braak to incorporate evidence that the first regions to be affected by Alzheimer’s are in the brainstem.
Indications that psychiatric disturbances occur prior to memory loss were proven when the teams from USP and UCSF compared the evolution of brain damage observed under the microscope with the psychiatric problems and clinical signs of Alzheimer’s exhibited by patients months before dying. Even in stages 1 and 2, when there are few lesions, which are concentrated in the structures of the brainstem such as the dorsal raphe nucleus and the locus coeruleus, signs of depression, anxiety, restlessness, and changes in appetite and sleep were more frequent.
The brainstem, which is considered one of the more primitive regions of the encephalon, connects the spinal cord to the brain. In the history of evolution, it first appears in amphibians, and in humans, it takes the form of an inverted cone that is 10 cm in length. The brainstem has less than 1% of the 86 billion neurons of the encephalon—neurons are the cells that transmit, process, and store information. However, it houses various small structures that perform functions that are fundamental to life. They participate in controlling respiration, hunger, heart beats, blood pressure, and body temperature, as well as regulating sleep-wake cycles. They also connect with regions of the brain that regulate humor, anxiety, and the formation and retrieval of memories.
Some of these structures have special neurons that produce more than one neurotransmitter, the compound that is responsible for communication among brain cells. “Through their neurotransmitters, these structures increase or decrease activity in many areas of the brain,” explains Nitrini, coauthor of the current study and an expert in dementia.
The new findings may represent two breakthroughs in the study and treatment of Alzheimer’s. The first is that the early identification of psychiatric signs can help in the testing of new medications, allowing, during initial stages of the disease, the assessment of the performance of compounds being developed to stop or slow the progression of Alzheimer’s—today, the majority of clinical trials are carried out with individuals in advanced stages, without encouraging results. Furthermore, for some researchers, the psychiatric manifestations of Alzheimer’s may make it possible to begin using available medications at an earlier stage. In an article published in 2015 in the magazine Neurobiology of Stress, the team of biologist Elisabeth Van Bockstaele, from Drexel University in the United States, suggests that the use of antidepressants could protect the structures of the brainstem from lesions or restore the function of these structures.
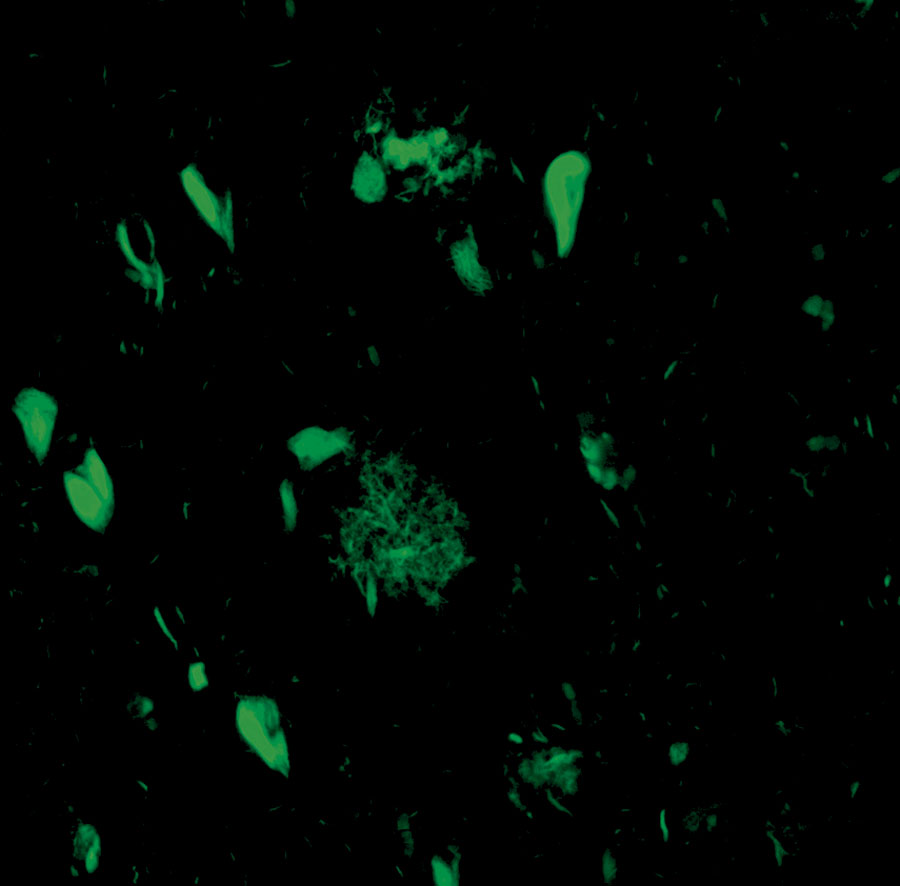
The structure that forms a web (center of the image) is a cluster of beta-amyloid plaques; the structures that form a candle flame are neurofibrillary tanglesCathrine Petersen / Lea T. Grinberg Lab / UCSF
“One of the important aspects of the study coordinated by Tenenholz Grinberg is that it shows that depression in seniors may not be initially caused by social or environmental factors, but rather, be the result of the degeneration of regions of the brain,” confirms psychiatrist Paula Villela Nunes, professor at the Jundiaí School of Medicine. This does not mean that it would be easier to treat these individuals. Villela Nunes, who is specialized in geriatric psychiatry and works as a researcher for the Psychiatric Institute (IPq) at USP, investigates the actions of compounds that are produced by the nervous system and protect the brain. However, she suspects that depression caused by Alzheimer’s will be less responsive to antidepressants due to the degenerative lesions in the brain. “Treating these cases of depression may be as challenging as treating dementia,” says Tenenholz Grinberg.
One of the brainstem structures first affected by Alzheimer’s is the locus coeruleus. This area contains noradrenergic neurons that produce noradrenaline, a neurotransmitter that controls interest, attention, stress, and other reactions to one’s surroundings. Changes in its functioning can cause sleep disturbances, anxiety, and depression, in addition to changes in memory and inflammation associated with the neurological lesions caused by Alzheimer’s. Another structure affected in the initial stages of the disease, which was identified by Tenenholz Grinberg and her team in 2009, is the dorsal raphe nucleus, an important center for serotonin production. Changes in the levels of this neurotransmitter are associated with depression and anxiety.
In the early stages of the disease, these structures exhibit only one of the two types of lesions described by Alois Alzheimer in 1906—he only published these findings in 1907, the year in which Oskar Fischer publicized his data. During a psychiatric conference in Tübingen, Germany, Alzheimer reported the case of Auguste Deter, a woman who was hospitalized in 1901 with an outburst of paranoia and who gradually exhibited sleep difficulties, memory loss, aggression, and confusion. She died five years later at 50 years of age, with the most external layer of the brain (cortex) covered by two types of lesions that became known as beta-amyloid protein plaques and neurofibrillary tangles of the tau protein—only the latter appeared in the locus coeruleus of the brains assessed by the USP and UCSF groups.
Recent analyses of postmortem brains and experiments with rats genetically altered to develop Alzheimer’s lesions suggest that the tangles of the tau protein are the first signs of damage to appear in the brainstem. Under normal conditions inside the cells, this protein plays the role of a wire that holds together a bundle of sticks: it encompasses and stabilizes groups of microtubules that define the cell’s structure. However, with Alzheimer’s, the protein is chemically changed, distorting it and freeing the sticks. Now untangled, they group together in an unorganized way, disrupting the function of the cell and sometimes killing it.
“The tangles are the first lesions that pathologists are able to observe, but I suspect they are not the triggers of the problem,” confirms biochemist Sergio Teixeira Ferreira, professor at the Federal University of Rio de Janeiro (UFRJ) and a specialist in the causes of Alzheimer’s. Like other experts, Ferreira perceives the origin of the problem in the abnormal degradation of the beta-amyloid precursor protein, which is essential to the survival of neurons, in the external surface of the cells. Various environmental factors—such as smoking, prolonged stress, or lack of sleep—seem to favor the detrimental dismantling of this protein, creating fragments called beta-amyloid peptides. These peptides tend to adhere to each other to form long fibers that, in turn, become the beta-amyloid plaques observed by Alzheimer in Auguste Deter’s brain.
In the mid-1990s, it was proposed that these plaques that accumulate outside the cells caused the death of a massive amount of neurons. However, it did not take long for doubts to arise. There were people whose brains were covered by plaques but they did not have dementia, while the opposite also occurred. In the last 20 years, increasing evidence has suggested that the most toxic effect is caused by smaller clusters: beta-amyloid oligomers, which produce both direct and indirect damage.
First, the beta-amyloid oligomers seem to block synapses (connections between neurons), leading the cells to atrophy or die. The oligomers also penetrate the neurons and alter the tau protein, facilitating the formation of the neurofibrillary tangles, which are also lethal for the cells. At UFRJ, Ferreira and neuroscientist Fernanda De Felice are helping to discover the toxicity of the oligomers, which can be partly indirect. In experiments with cells and animals, they have shown that oligomers cause an inflammatory reaction: they stimulate microglia, which are key defense cells for the central nervous system, to produce cytokines such as tumor necrosis factor alpha. These inflammatory mediators, in turn, make the neurons more sensitive to the destruction caused bythe oligomers.
Since Alzheimer’s characterization 112 years ago, tens of thousands of studies have been published, and dozens of compounds have been tested in an attempt to stop or slow the disease. Today, specialists predict that the solution lies in seeking ways of identifying lesions in the beginning or before they appear—brain imaging is being developed to detect the presence of oligomers in the brain—and using compounds that avoid damage before the appearance of clinical signs of the disease.
In January of this year, there were 112 compounds in one of the three phases of clinical testing on human beings who will take these medications prior to market availability. Of these compounds, 63% seek to change the course of the disease, according to assessments carried out by neurologist Jeffrey Cummings of the Cleveland Clinic in the United States, and published in the journal Alzheimer’s & Dementia. In general, they are antibodies, biological molecules that adhere to the beta-amyloid peptides, to the tau protein, or to both, and neutralize them. When used in the advanced stages, they are not very effective, but there are an increasing number of attempts to test them in people without symptoms of Alzheimer’s disease or those who have a higher risk of developing the disease. One of these studies is being carried out in Colombia by neurologist Francisco Lopera, professor at the University of Antioquia. He and his colleagues are using the monoclonal antibody crenezumab to treat 100 individuals from families who carry a genetic modification that accelerates the production of beta-amyloid and leads to dementia prior to 50 years of age. These participants will take the medication for five years, after which their results will be compared with those of individuals who took a placebo—the first data should be available in 2022. “For people without symptoms, upon beginning treatment, we expect greater success in the neutralization of the amyloid,” reports Lopera to Pesquisa FAPESP. “It may also be necessary to use antibodies that block the tau protein.”
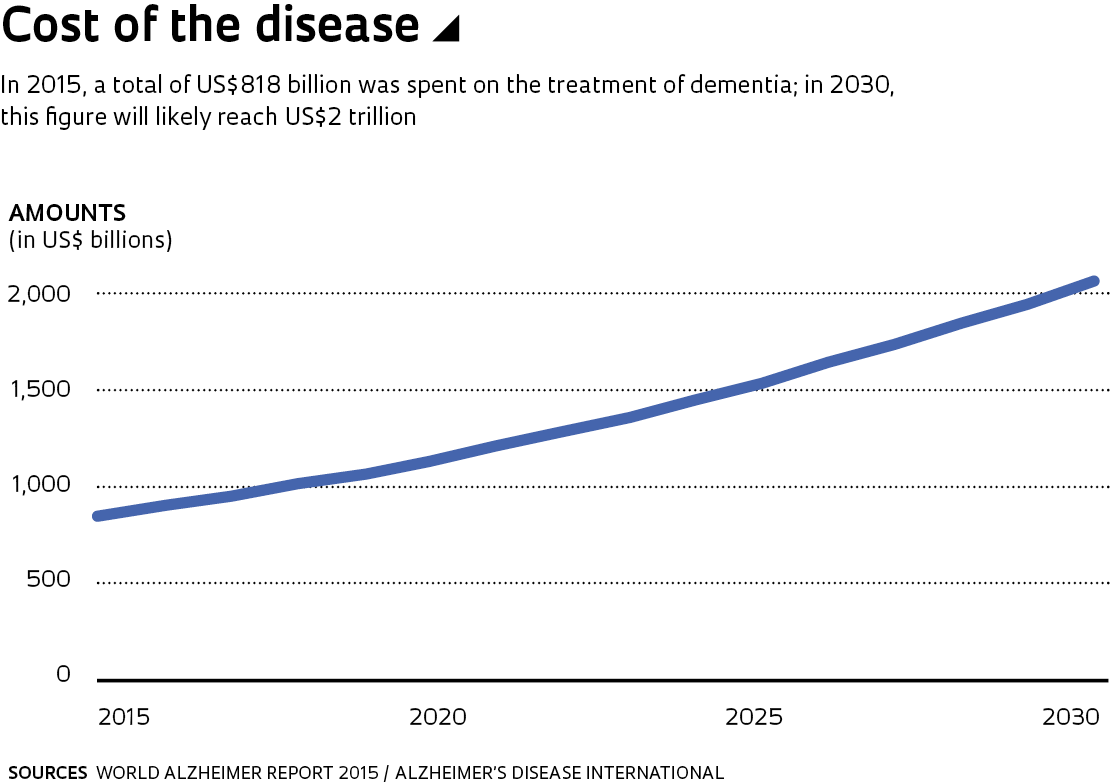
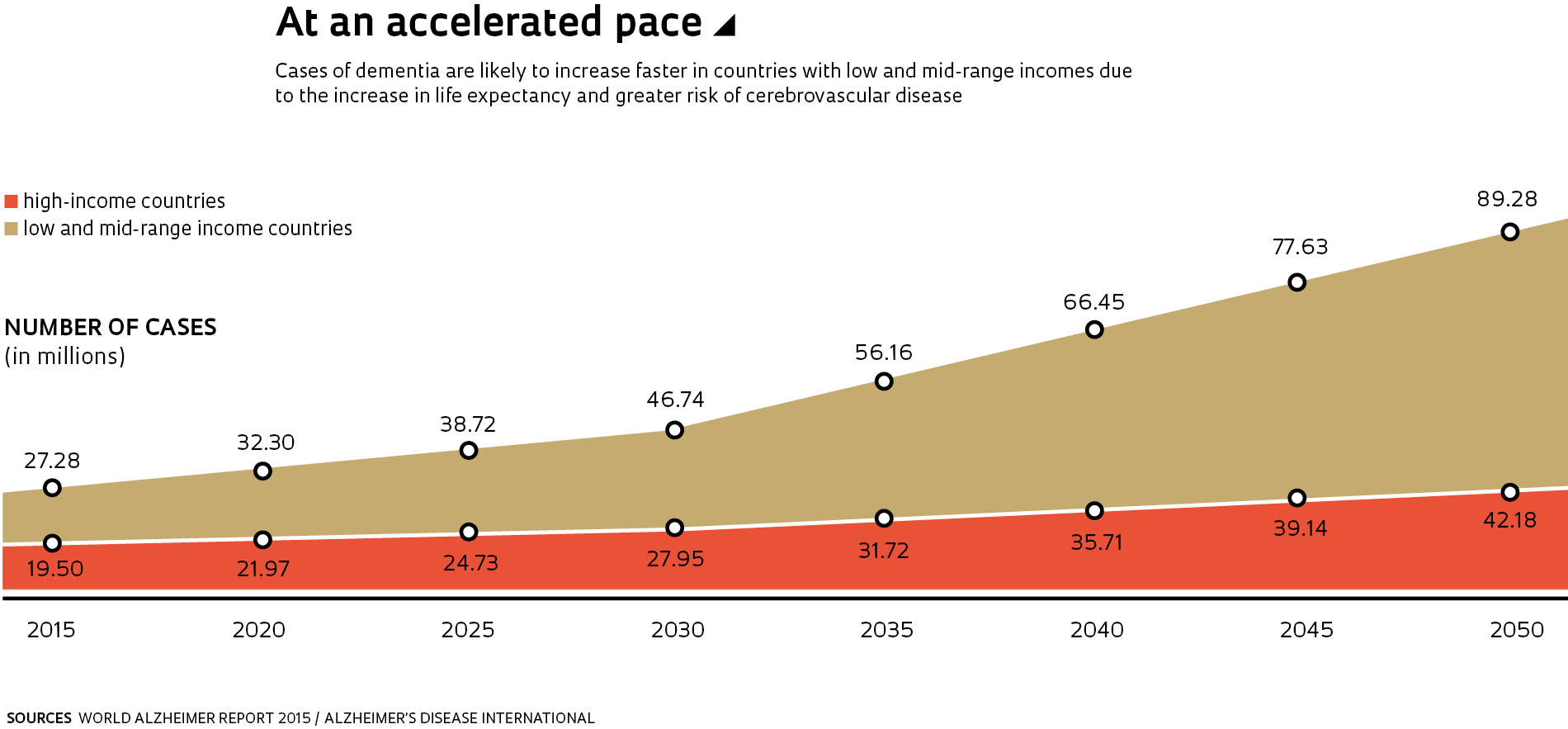
There is an urgent need to find effective treatments for Alzheimer’s. The compounds used to slow memory loss act on the neurotransmitter acetylcholine and increase attention. However, they only work for a few years at most. Furthermore, the disease is becoming more common as people live longer. The World Health Organization calculates that there are almost 50 million people with dementia around the world, with 60% to 80% of cases resulting from Alzheimer’s. This number should triple by 2050 (see graph above). Taking care of people with dementia costs US$818 billion per year worldwide, according to the World Alzheimer Report 2015, published by the nongovernmental organization Alzheimer’s Disease International. In Brazil, the treatment of each individual costs an average of US$16,500 per year, as shown in data published this year by researchers from USP, the University of Taubaté, and the Santa Marcelina Hospital in PLOS ONE. Approximate calculations suggest that there are 1.2 million individuals with dementia throughout the country and that 100,000 new cases arise each year.
Published in November 2018
Project 1. Diagnóstico nosológico de demência em população brasileira (nº 06/55318-1); Modalidade Auxílio à Pesquisa – Regular; Pesquisador responsável Ricardo Nitrini (USP); Investimento R$ 123.173,15 2. Caracterização das alterações da proteína TDP-43 durante o envelhecimento normal: uma análise de cérebros post mortem (nº 11/19833-7); Modalidade Bolsa de Doutorado; Pesquisador responsável Lea Tenenholz Grinberg (USP); Bolsista Camila Nascimento Mantelli; Investimento R$ 105.846, 60 3. Análise proteômica dos grânulos de neuromelanina no envelhecimento normal e na doença de Parkinson (nº 10/06521-4); Modalidade Bolsa de Pós-doutorado; Pesquisador responsável Lea Tenenholz Grinberg (USP); Bolsista Renata Elaine Paraizo Leite; Investimento R$ 223.946,46 4. Doença por grãos argirofílicos (nº 12/07526-5); Modalidade Bolsa de Doutorado Direto; Pesquisador responsável Lea Tenenholz Grinberg (USP); Bolsista Roberta Diehl Rodriguez; Investimento R$ 46.896,43
This article may be republished online under the CC-BY-NC-ND Creative Commons license. The Pesquisa FAPESP Digital Content Republishing Policy, specified here, must be followed. In summary, the text must not be edited and the author(s) and source (Pesquisa FAPESP) must be credited. Using the HTML button will ensure that these standards are followed. If reproducing only the text, please consult the Digital Republishing Policy.