 EDUARDO CESARBrazil is finally beginning to find out the magnitude of a severe health problem that experts refer to as the silent disease: the viral hepatites, illnesses that produce the same clinical signs, although they are caused by different types of viruses lodged in the liver, which trigger inflammation that harms this organ. On Thursday, July 28, World Hepatitis Day, the Ministry of Health released the results of the broadest survey of these diseases ever conducted in Brazil. For seven years, a battalion of almost one thousand researchers headed by the hepatologist Leila Beltrão Pereira and by epidemiologist Ricardo Ximenos, both from the University of Pernambuco (UPE), and by the biomedical researcher Regina Moreira, from the Adolfo Lutz Institute, in São Paulo, interviewed and took blood samples from 26,102 people in all Brazilian state capitals and in the country’s capital, Brasilia.
EDUARDO CESARBrazil is finally beginning to find out the magnitude of a severe health problem that experts refer to as the silent disease: the viral hepatites, illnesses that produce the same clinical signs, although they are caused by different types of viruses lodged in the liver, which trigger inflammation that harms this organ. On Thursday, July 28, World Hepatitis Day, the Ministry of Health released the results of the broadest survey of these diseases ever conducted in Brazil. For seven years, a battalion of almost one thousand researchers headed by the hepatologist Leila Beltrão Pereira and by epidemiologist Ricardo Ximenos, both from the University of Pernambuco (UPE), and by the biomedical researcher Regina Moreira, from the Adolfo Lutz Institute, in São Paulo, interviewed and took blood samples from 26,102 people in all Brazilian state capitals and in the country’s capital, Brasilia.
The situation revealed in this study became even more clearly defined thanks to the recent findings of other Brazilian teams. Instead of surveying the rate of infected individuals in the population, the group of the physician and biochemist João Renato Rebello Pinho at the University of São Paulo (USP) looked for communities throughout the country known to have a high ratio of infection, to map the varieties of viruses that are circulating. Another piece of research, in which researchers from the State University of Campinas (Unicamp) and from the Federal University of Rio de Janeiro (UFRJ) took part, projected the evolution of the ratios of hepatites up to the end of this decade. When taken together, these results can provide better guidance on how best to fight these hepatites.
The preliminary conclusions of the population survey, i.e., the Inquérito nacional de prevalência de hepatites virais [National survey of the prevalence of viral hepatites] reveal a better picture than that previously reported by the World Health Organization (WHO). The international agency classified Brazil as having a high concentration of hepatitis A cases; a low number of hepatitis B cases, except for the North region, where it was high; and an intermediate level of hepatitis C cases. According to the study commissioned by the Ministry, the prevalence of the three most common forms of hepatitis fluctuates from moderate (the case of A in the North, Northeast, and Midwest areas) to low, as is the case of B and C, which are less frequent and more aggressive. “This research study changed the map of hepatitis in Brazil,” states Leila, who coordinated the research. “The concentration of cases is only high in the Amazon region, and even so just in certain regions, such as around the Javari River [on the Brazil-Peru border],” she says.
 An analysis of the blood of 6,468 children and adolescents showed that, on average, 39.5% had antibodies against the hepatitis A virus, the most frequent one worldwide, affecting 1.4 million people every year. Detecting this antibody is an indication that these individuals have already come into contact with the agent that causes the disease, though it does not mean that they were ill at the time of the research. Transmitted by the consumption of contaminated water and foods, the hepatitis A virus does not harm the organism of children and of adolescents severely. About half the infected people do not even show signs of the disease. Among the other half, following an incubation period of 15 to 45 days, the virus can cause fever, malaise, abdominal discomfort, yellowing of the skin and eyes (jaundice) and urine the color of Coca-Cola, due to a passing liver inflammation. The virus is almost always eliminated from the body with no specific treatment other than rest, though there are rare cases, usually among adults, in which the infection progresses aggressively, leading to death in a few weeks (see table). Once the acute stage of the infection is over, the person becomes immune to the virus.
An analysis of the blood of 6,468 children and adolescents showed that, on average, 39.5% had antibodies against the hepatitis A virus, the most frequent one worldwide, affecting 1.4 million people every year. Detecting this antibody is an indication that these individuals have already come into contact with the agent that causes the disease, though it does not mean that they were ill at the time of the research. Transmitted by the consumption of contaminated water and foods, the hepatitis A virus does not harm the organism of children and of adolescents severely. About half the infected people do not even show signs of the disease. Among the other half, following an incubation period of 15 to 45 days, the virus can cause fever, malaise, abdominal discomfort, yellowing of the skin and eyes (jaundice) and urine the color of Coca-Cola, due to a passing liver inflammation. The virus is almost always eliminated from the body with no specific treatment other than rest, though there are rare cases, usually among adults, in which the infection progresses aggressively, leading to death in a few weeks (see table). Once the acute stage of the infection is over, the person becomes immune to the virus.
“Twenty years ago, the proportion of children and adolescents infected by the hepatitis A virus was 90%,” the hepatologist Flair José Carrilho tells us. A senior professor of gastroenterology at the USP School of Medicine, he is responsible for the part of the survey that was conducted in São Paulo state.
One of the reasons why the rate of hepatitis A has dropped, according to the government, is better basic sanitation. The number of houses with treated water increased from 78% to 83% in the last decade and the number of homes connected to the sewage system, from 47% to 55%, as shown by a comparison between the 2000 census and 2010 census of the Brazilian Institute of Geography and Statistics (IBGE).
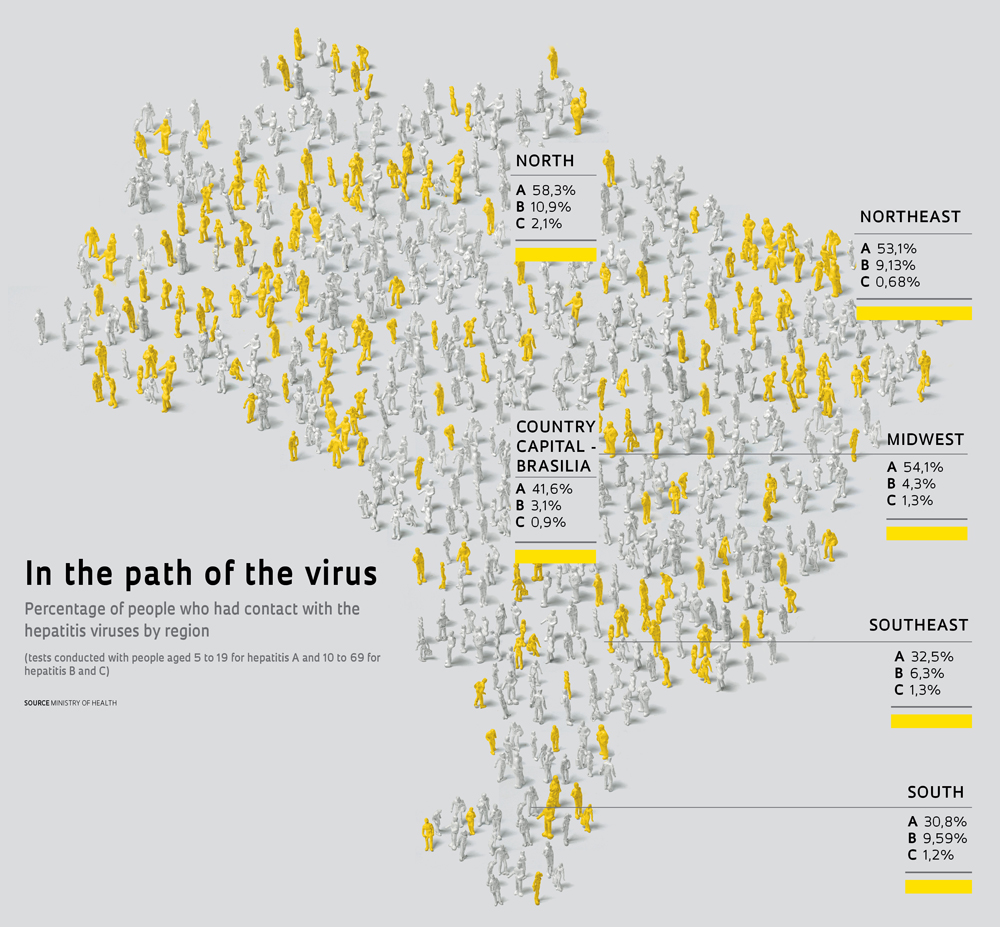
The distribution of the hepatitis A cases, as one can imagine, is not homogeneous. The frequency increases from the south toward the north of Brazil – from 31% in the southern capital cities to 58% in the capitals of the North region – where the water and sewage collection system is smaller. “These figures show the influence of access to sanitation, which is smaller in these capitals and favors the dissemination of the virus,” notes Dirceu Greco, director of the Department of Sexually Transmitted Diseases, Aids and Viral Hepatites of the Ministry of Health. At present, technicians from the ministry and experts from several regions are assessing the costs and benefits of including the hepatitis A vaccine in the National Immunization Program. Currently, the vaccine is only distributed in high-risk areas. “With a reduction of the prevalence of this hepatitis among children and young people, there is a risk that people are infected later in life, when the possibility of complications increases,” says Greco.
 The situation becomes more complex when one analyzes the data for hepatitis B and hepatitis C. The researchers measured the presence of three proteins indicating infection by the B virus and one by the C virus in the blood of 19,634 participants. They found that 7.4% of these people had already been contaminated by the B virus, although only 0.4% suffered from hepatitis at the time of the research, and that 1.4% had contracted the C virus.
The situation becomes more complex when one analyzes the data for hepatitis B and hepatitis C. The researchers measured the presence of three proteins indicating infection by the B virus and one by the C virus in the blood of 19,634 participants. They found that 7.4% of these people had already been contaminated by the B virus, although only 0.4% suffered from hepatitis at the time of the research, and that 1.4% had contracted the C virus.
At first, these figures seem more encouraging than those of the WHO, but the lower rates of hepatitis may not be very significant. The WHO documents were based on old data from studies involving few people – generally, blood donors – and conducted in limited areas. “The result of the national survey do not surprise the physicians,” states Fernando Gonçales Junior, from Unicamp. “Tests in blood banks had already indicated an active infection rate of 0.5% for hepatitis B and of 1.4% for hepatitis C,” he tells us.
In a study conducted jointly with foreign researchers and with the gastroenterologist Henrique Coelho, from UFRJ, Gonçales gathered information from 150 Latin-American scientific articles on hepatitis and data supplied by the healthcare systems of four countries (Argentina, Brazil, Mexico and Puerto Rico) to feed a mathematical model that might project the evolution of hepatitis C in upcoming years. The trend, described in an article in the July issue of Liver International, is that the total number of cases will increase, while the ratio will remain stable (at 1.5% in the case of Brazil) until 2021.
The limitation of the national survey, according to the experts, is that it only covered the population of the state capitals and of the country’s capital, though the sample is large and represents one quarter of all Brazilians. “The survey is very valuable because it maps these diseases nationwide, but one cannot forget that the determinants of these diseases are socioeconomic and environmental factors, especially when it comes to hepatitis A,” states Rosangela Gaze, a sanitation doctor from the Laboratory of History, Health and Society of the UFRJ Medical School. “The frequence of this hepatitis can vary a lot, even in the capitals,” say the researchers.
Assuming the ratios of this survey can be extrapolated to the entire population, then it would seem that there are 3.5 million Brazilians suffering from the more severe forms of hepatitis (some 800 thousand with hepatitis B and 2.7 million with hepatitis C), six times the estimated number of people with Aids. “It really is a large number,” acknowledge Greco, from the ministry. Together, the people with these two forms of hepatitis, whose risk of developing cirrhosis and cancer of the liver over the course of their lives is greater, would be equivalent to a city the size of Salvador, in Bahia state, and the country’s third largest. “These data will generate a major discussion about the financing of treatment for hepatitis, which is quite expensive,” states Carrilho. “The Single Healthcare System is unable to foot the bill for all of this,” he adds.
Luckily, not all infected people need treatment. International studies that tracked the natural evolution of the various hepatites have shown that as many as 90% of the people who contract the B virus have an acute inflammation lasting only a few weeks and manage to control the proliferation of the virus without developing chronic hepatitis. Nevertheless, the number of people that require medication is still high: about 160 thousand. Among those affected by the C virus, for which treatment is less effective, the number is almost 10 times as high, as only in 20% of the cases does the infection fail to become chronic.
However, only a few people discover the illness and get to the public health services – generally after the problem has advanced and the clinical signs have become evident. “These cases are usually more serious, with less chance of a cure,” says Carrilho. In the last decade, the Ministry recorded 104 thousand cases of hepatitis B and 70 thousand of hepatitis C (see table) and in 2010 it spent some R$250 million to R$300 million treating 24 thousand people with one of these two types of hepatitis.
 One of the reasons why the disease goes undiagnosed is that the evolution of hepatitis B and hepatitis C is very slow. Twenty to 30 years can go by before the liver, a sponge-like organ that is soft to the touch, starts hardening due to cirrhosis, the healing of the lesions caused by the virus and by the body’s defense system. At this stage, varicosity usually appears in the stomach and the esophagus, the skin may develop small web-like veins and the risk of hemorrhages increases. “Professor Luiz Caetano da Silva, one of the pioneers of hepatology in Brazil, used to say that the liver suffers in silence,” recalls Carrilho, who was a doctoral student under Silva.
One of the reasons why the disease goes undiagnosed is that the evolution of hepatitis B and hepatitis C is very slow. Twenty to 30 years can go by before the liver, a sponge-like organ that is soft to the touch, starts hardening due to cirrhosis, the healing of the lesions caused by the virus and by the body’s defense system. At this stage, varicosity usually appears in the stomach and the esophagus, the skin may develop small web-like veins and the risk of hemorrhages increases. “Professor Luiz Caetano da Silva, one of the pioneers of hepatology in Brazil, used to say that the liver suffers in silence,” recalls Carrilho, who was a doctoral student under Silva.
The Ministry is trying to expand early diagnosis, with campaigns for doing tests. In August, it started distributing fast diagnosis kits for hepatitis B and hepatitis C to 17 public centers. These kits reduce the amount of time it takes to get the results from two weeks to just half an hour. This year, the four largest blood centers in Brazil (São Paulo, Rio de Janeiro, Santa Catarina and Pernambuco) began assessing the Brazilian version of a molecular test to identify the hepatitis C virus in blood, rather than identifying antibodies to it, which remain in the organism even after the virus has been eliminated. Developed by the team of Antonio Gomes Pinto Ferreira and Marco Aurélio Krieger, from the Oswaldo Cruz Foundation (Fiocruz), together with the Institute of Technology of Paraná and Empresa Brasileira de Hemoderivados e Biotecnologia (a blood products and biotechnology concern), the test is produced by Bio-Manguinhos, the Immunobiological Technology Institute of Fiocruz, and it should cut the time diagnosis takes from 70 days to 10.
The risk of hepatitis C contamination due to blood transfusions is low in Brazil, Ester Sabino tells us. She heads the department of molecular biology of the Pró-Sangue/Hemocentro Foundation of São Paulo. One out of every 200 thousand blood bags is infected with the virus. However, Ester believes that using the molecular test will produce the same effects as it did in the United States, where it has been employed since 2000: slash the infection rate to one bag out of every million.
“As more sensitive and specific tests are developed, the hepatites become more visible and are detected more often,” says Rosangela, who, in her doctoral studies, investigated the influence of technological changes on the diagnosis of hepatitis in the eighteenth and nineteenth centuries by studying the academic theses of the Rio de Janeiro Medical School, now part of UFRJ. “But there hasn’t been the same evolution in terms of treatment and prevention,” she states.
Five or six drugs are used – combined or individually – to treat serious hepatitis. To fight B, physicians usually prescribe lamivudine, adefovir, tenofovir or entecavir, which may or may not be associated with a compound that imitates interferon, an antiviral molecule produced naturally by the body. In most cases, these compounds control the reproduction of the virus efficiently, but do not rid the organism of it. This is the case because the hepatitis B virus sometimes inserts a segment of its genetic material (DNA) among the genes of the infected cell and takes over control. Thus, it can stay dormant in some of them and years later become active again, which is why many carriers of the B virus get hepatitis again after a liver transplant.
The treatments that work on hepatitis B, however, do not always work to fight C, which is more aggressive and lethal. One of the strategies used most often to fight hepatitis C is the association of interferon and of the antiviral drug ribavirin. This combination, which only cures 40% of the infections caused by some varieties of the C virus, is to be reinforced, in the next few months, by another two compounds: telaprevir and boceprevir, both of which have been approved for sale by the National Sanitary Surveillance Agency (Anvisa). In clinical trials, they raised the success ratio of treatment to 70%.
Underlying the partial success of these treatments are the genetic characteristics of the hepatitis virus, which vary a lot. Since the identification by Baruch Blumberg, in 1965, of the first viral agent for hepatitis – the B virus – another five types have been described: A, C, D and G (see table). However, the subtleties do not stop here. The sophistication of diagnostic methods has enabled doctors to differentiate subtypes within each type – the genotypes, described by numbers or upper case letters. Then there are the subtypes: the sub-genotypes, represented by numbers or lower case letters.
 For the last six years, the team of João Renato Rebello Pinho, from the Laboratory of Gastroenterology and Tropical Hepatology of the Institute of Tropical Medicine of the USP School of Medicine has been working on the identification of the genotypes and sub-genotypes of the viruses found in Brazil and in other South American countries. The objective is to find out which varieties are circulating here and where they are found. The data produced to date, described in almost a dozen scientific articles, refine the knowledge of hepatitis in South America and should help to reconstitute the history of the evolution of the B and C viruses on this continent.
For the last six years, the team of João Renato Rebello Pinho, from the Laboratory of Gastroenterology and Tropical Hepatology of the Institute of Tropical Medicine of the USP School of Medicine has been working on the identification of the genotypes and sub-genotypes of the viruses found in Brazil and in other South American countries. The objective is to find out which varieties are circulating here and where they are found. The data produced to date, described in almost a dozen scientific articles, refine the knowledge of hepatitis in South America and should help to reconstitute the history of the evolution of the B and C viruses on this continent.
“We hadn’t expected to find such a wide variety,” states the Colombian microbiologist Mónica Viviana Alvarado-Mora, a doctoral student supervised by Pinho. Together with teams from other regions in Brazil as well as from Chile, Colombia and Venezuela, Pinho’s group identified in South America, for the first time, a variety of the hepatitis B virus that was previously thought to exist only in Africa: the B virus, E sub-genotype, found in Quibdó, a community of Afro-descendants in western Colombia. Molecular tests that calculate the rate of accumulation of mutations in the genetic material over time suggest that this variety of virus was introduced only once in this area of South America, though it is not known when this occurred.
Crossing Colombia, Mónica collected blood samples from communities in four different regions and, for the first time, identified the rate of prevalence of hepatitis and the most common genotypes of the B and C viruses in the country. Among the B viruses, she found two of the four varieties of the F genotype, the most common one among the Amerindians, and one of the G genotype, according to an article published this year in Infection, Genetics and Evolution. She also saw something unexpected: the high prevalence of sub-genotype A2, typical of Europeans, in Bogotá, the capital. As for the C virus, the most common variant was the 1b type, indicating that in Colombia transmission of this type of hepatitis is due mainly to the transfusion of infected blood rather than to the use of injectable drugs. “The infection rate has been dropping since the blood banks started using tests to detect the C virus,” she states.
The group has also found evidence that vaccination against hepatitis B is effective in Brazil. “The immunization against the B virus has reduced the prevalence of the virus of the Delta [or D] hepatitis virus, genotype 3, only found in the Amazon Region,” says Mónica. Unlike the other viruses, D is defective and only invades cells infected by the B virus. “This information is important in order to determine the best treatment strategy and for the development of more specific diagnostic tests,” states Pinho.
The most effective measure, however, is to protect oneself from contagion as much as possible. One of the ways is to avoid contact with blood and other bodily fluids, use condoms during sexual intercourse and clean day-to-day objects properly, such as clippers and cutlery. As much as 100 times more infectious than the Aids virus, the hepatitis B virus is present in the blood, the semen and the saliva. The most frequent form of transmission in Brazil is sex with no condom, though it can also result from sharing personal objects or a mere kiss.
Another way to avoid hepatitis B is vaccination. “A safe and effective hepatitis B vaccine has been available since the 1980’s,” Rosangela recalls, “but in Brazil we still vaccinate a lot fewer people than we could.”
Since 1998, the National Immunizations Program recommends vaccination soon after birth. Today, 85% of Brazilian children of up to 18 months of age receive the three doses. However, this rate drops to less than 30% among adolescents, who are about to start their sex life. “Many take the first dose, but don’t take the others,” comments Gonçales, from Unicamp. In Rosangela’s opinion, one should put in place strategies to remind the population. “Hepatitis B is carried more easily than other sexually transmitted diseases and we can’t expect people to remember to have all the doses,” she says.
The marketing of a hepatitis B vaccine developed by the Butantan Institute, in São Paulo, cut from US$90 to R$1.5 the cost of the three doses. This year, the Ministry expanded the age group for free vaccination to 24 years of age and, starting in 2012, the vaccine will be offered to people up to the age of 29. “We want to immunize the entire population of this age group,” says Greco.
As for hepatitis C, there is no vaccine yet. However, results presented in August 3 in Science Translational Medicine provide some hope. The group of David Klatzmann, from the Pierre and Marie Curie University in France, has reached a possible strategy for the production of a recombinant vaccine. The researchers inserted copies of the genes of the hepatitis C virus into the measles virus and applied this to mice and monkeys. The organisms of the rodents and of the primates then produced antibodies against a broad variety of hepatitis C viruses.
The projects
1. Study of the genotypical variability of the viruses of the hepatites B and C in Colombia (nº 2007/53457-7); Modality Regular Research Award; Coordinator João Renato Rebello Pinho – IMT/USP; Investment R$ 260,277.97 (FAPESP).
2. Study of the genetic diversity of the hepatitis C virus and the hantavirus circulating in the state of São Paulo (nº 2000/11457-1); Modality Regular Research Award; Coordinator João Renato Rebello Pinho – IMT/USP; Investment R$ 1,169,490.33 (FAPESP).
3. Study of the prevalence and genotyping of the hepatitis B virus in the state of Paraná, Brazil (nº 1999/09551-0); Modality Regular Research Award; Coordinator João Renato Rebello Pinho – IMT/USP; Investment R$ 129,862.29 (FAPESP).
Scientific articles
KERSHNOBICH, D. et al. Trends and projections of hepatitis C virus epidemiology in Latin America. Liver International.
NAKATANI, S. M. et al. Development of hepatitis C virus genotyping by real-time PCR based on the NS5B region. PLoS One. v. 5 (4). Apr. 2010.
ALVARADO-MORA, M.V. et al. Molecular epidemiology and genetic diversity of hepatitis B virus genotype and in an isolated Afro-Colombian community. Journal of General Virology. v. 91, p. 501-8. 2010.