Experimental therapy tested for the first time in Brazil uses a patient's own defense system to fight cancer
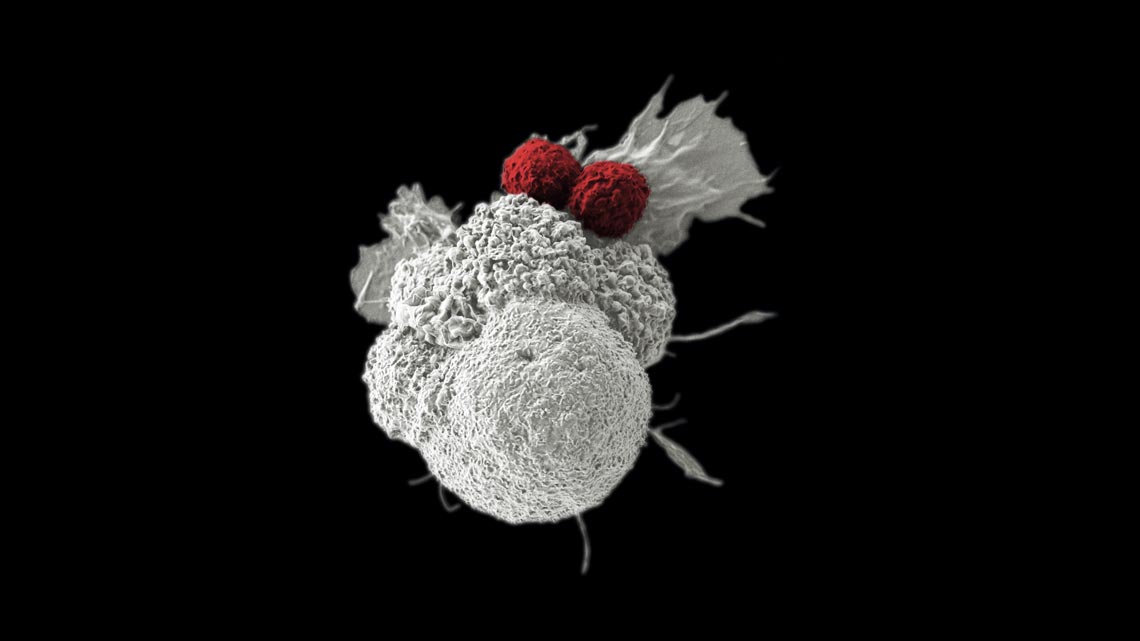
Electron microscopy shows tumor cell (in white) under attack by two artificially colored T cells (in red)
Rita Elena Serda/National Cancer Institute (NCI)/Duncan Comprehensive Cancer Center at Baylor College of Medicine
Vamberto Luiz de Castro did not expect he would live much longer when he arrived at the Hospital das Clínicas of the University of São Paulo in Ribeirão Preto (USP-RP) this past August. He had advanced cancer and had lost almost 20 kilos over the previous months. In 2017, the retired civil servant from Belo Horizonte had been diagnosed with lymphoma due to a proliferation of B lymphocytes (B cells). In healthy people, these cells produce antibodies that counter viruses, bacteria, and other elements foreign to the body. In people with cancer, however, they start to multiply uncontrollably. The doctors who initially treated Castro tried to fight the disease with drugs and radiation, but when the treatments were ineffective they gave him one year to live. The retiree from Minas Gerais was under palliative care, receiving morphine to endure the pain, when his son Pedro Augusto learned of an innovative, risky treatment that would soon be offered experimentally in Brazil.
In Ribeirão Preto, researchers led by hematologist Dimas Tadeu Covas had recently developed a therapy that was still unprecedented in Latin America. They were preparing to offer it as compassionate therapy (offered when other treatment alternatives have been exhausted) for people with two types of cancer. One of them was the type killing Castro. Its name is complicated: chimeric antigen receptor T lymphocyte therapy, or, in its trimmer version, CAR-T cell therapy.
In this treatment, the medical team extracts one type of defense cell—T lymphocytes, or T cells—from the patient’s own blood, in order to avoid rejection later. These cells are then genetically modified in the lab to identify and destroy tumor cells. In healthy individuals, T cells naturally recognize and eliminate diseased cells, such as tumor cells. However, tumor cells sometimes escape the body’s sentinels. Over the past 30 years, scientists have discovered how to lend T cells a helping hand with this task. They only need to insert the instructions for making a certain protein into the T cell genome. This protein sits exposed on the T cell’s outer surface, and has an affinity for the cells that need to be destroyed. The strategy works well against B cells.
Recently mastered by the USP group, the treatment is a promising way to fight tumors caused by the proliferation of B cells that are resistant to chemotherapy and radiation treatment. Its viability was first demonstrated by Israeli immunologist Zelig Eshhar, in 1989. Since then, groups in the United States have perfected cell manipulation, and the treatment’s safety, which was first tested on humans about 10 years ago. The development of treatment variations took off in 2013, and today there are about 680 versions at different stages of development.
Despite this explosion of possibilities, only two therapies using CAR-T cells are available for commercial clinical use. One treats a type of leukemia (blood cancer) and the other fights lymphomas, which both result from a proliferation of B cells.
The first treatment was developed at the University of Pennsylvania, in the United States. This therapy was approved by the FDA, the US drug regulatory agency, to treat acute B cell lymphoblastic leukemia that resists conventional drugs. There, the treatment, called Kymriah, costs US$475,000, not including hospital costs. A review published in 2018 in the New England Journal of Medicine indicates that the cancers in 70% to 90% of people treated go into remission shortly after therapy. Over time, 25% will have their leukemia return.
The second treatment, created at the National Cancer Institute (NCI) in the United States and marketed under the name Yescarta, works against B cell lymphomas that won’t yield to traditional therapies, as was the case with Vamberto Castro. It costs US$370,000, still a prohibitive sum for many who could benefit from it. Between 65% and 85% of people with large B cell lymphoma initially show a reduction in tumors, but only half of them experience a complete, lasting response.
As none of the therapies is approved in Brazil, one alternative for Castro would have been to seek treatment abroad. The problem was the cost. The procedure would have cost almost US$1 million, the retiree told the O Globo news podcast in October, days after being discharged from the USP Cellular Therapy Center (CTC) in Ribeirão Preto, where he had been treated with CAR-T cells.
“By 2018, our group had already mastered the production cycle for these cells and we were ready to treat our first patients,” says Covas, coordinator of the CTC, one of the Research, Innovation and Dissemination Centers (RIDC) supported by FAPESP, and the current director of the Butantan Institute. “There are few places in the world with the capacity to provide this treatment.” Out of prudence, the team postponed the offer of compassionate therapy until hematologist Renato Cunha returned from NCI, where he spent a season learning to manage its side effects, which are intense and can lead to death.
Once injected into the blood, CAR-T cells start the hunt. When they find a B cell, they adhere to it and launch a bath of chemical compounds (cytokines) that kill it, whether it’s a healthy cell or a tumor cell. Necessary in order to eliminate the tumor cells, this chemical bath—called a cytokine storm—is a sign that the treatment is working. At higher levels, however, these compounds lower blood pressure and cause fluids to leak into the organs.
“One worrisome adverse effect is cerebral edema,” notes American immunologist Kenneth Gollob, head of the Translational Immuno-oncology Group at the A.C.Camargo Cancer Center, in São Paulo, which is seeking new targets for CAR-T cells. “In order to deal with these effects, a well-prepared clinical team is required, in addition to quick access to an intensive care unit and drugs to control the side effects of the cytokine storm,” adds Covas.
When Castro went to his first consultation in Ribeirão Preto, the CTC group already had T cells from other patients prepared for the first treatment. The seriousness of his case, however, led doctors to change the order of the procedures. The lymphoma had progressed rapidly and moved into his bones. The patient was experiencing excruciating pain and intermittent fever, as well as night sweats that soaked his clothes and bed. “At this stage, the tumor cells reproduce so quickly and have such a high metabolism that it’s as if the patient were doing intense physical activity while sleeping,” reports Covas.
The decision to offer treatment had been preceded by long preparation. Established two decades ago, the CTC has extensive experience with bone marrow transplants, and has been a pioneer in Brazil in the use of stem cells to treat autoimmune diseases, such as Type 1 diabetes. Continuous improvements in the production of CAR-T cells, and promising results with in vitro and animal tests, followed by the first successful cases in humans convinced CTC researchers to invest in mastering the steps necessary to independently create their own production line of CAR-T cells.
One method of producing these cells requires the use of viruses. It is the viruses that insert the genes into the T cell genome, genes that carry instructions for making proteins that will direct the T cells against B cells. In general, every research group or pharmaceutical company develops a production strategy and patents its work stages, or maintains them as trade secrets. For this reason, the USP team chose to create its own virus. “Initially, we thought about buying the viruses from US laboratories,” says biologist Virginia Picanço e Castro of the CTC, coauthor of the book Chimeric Antigen Receptor T Cells, to be published in 2020 by Humana Press. “Since importing is complex and expensive, we decided to develop this stage here.”
It took four years of work, including training abroad, to master the steps in viral vector production and multiplying the genetically modified T cells. Picanço e Castro spent time at Purdue University in the United States, learning how to prepare the virus, while chemist Amanda Mizukami went to the University of Washington to train in cultivating genetically modified T cells. Both stages are essential in developing the therapy and, on their return to Brazil, the researchers implemented them in Ribeirão Preto.
At USP, Picanço e Castro and her team learned how to generate a harmless version of the human immunodeficiency virus (HIV) to insert genes into T cells. Biotech engineer Pablo Moço produced a variant of the virus free of the genes that make it dangerous, while Mariane Tirapelle, also a biotech engineer, worked to improve production and make it cheaper. After incorporating the genes to be inserted in the T cells into the virus’s genetic material, it was up to Mizukami to multiply the genetically modified cells in the lab. In their in vitro tests, the CTC’s CAR-T cells eliminated 90% of the B cells in one day. According to results published in October in the journal Hematology, Transfusion and Cell Therapy, they also controlled B cell lymphoma in mice.
“This fundamental technological step was made possible because we already had expertise in assembling and manipulating viral vectors, and in culturing cells in bioreactors, all following best practices for manufacturing required for therapy in humans, which was developed for performing bone marrow transplants,” Covas says. “We mastered the entire cycle, and we were only able to do so in the public health sector because of the research investment made by funding agencies such as FAPESP and the National Council for Scientific and Technological Development [CNPq].” In all, 20 people from RIDC worked to develop the treatment: five doctors, five researchers, seven graduate students and postdoctoral interns, and three lab technicians.
In early August, the CTC medical team collected T cells from Vamberto Castro and sent them to the laboratory to be genetically manipulated. About 40 days later, on September 9, the retiree was readmitted to have his cells returned, now transformed into CAR-T cells. Two days after the infusion, the effect started to become apparent: it was possible to reduce the morphine, and the cytokine storm began. Castro went into shock. His blood pressure dropped and it became necessary to hydrate him, in addition to administering antibodies to control the cytokines. Four days later, he had improved and was taken to the nursing ward. “One month after the infusion there was no more evidence of neoplastic B cells in his blood and imaging tests showed a drastic reduction in lymphoma,” says Covas.
On October 11, Castro was discharged and went home. Considered to be in clinical remission and given a favorable prognosis, his case will be followed by the Ribeirão Preto doctors over the coming years. The protection of the CAR-T cells should last as long as they remain alive in his body. Some people who undergo treatment, however, may have their tumors recur, either because the CAR-T cells become inactive, or because the neoplastic cells undergo changes that allow them to circumvent the genetically modified lymphocytes.
“The results in this case are an important indication that the therapy works,” says biomedical doctor Martín Bonamino, from the National Cancer Institute (INCA), in Rio de Janeiro. “Since the treatment is recent, it’s too early to know if there will be a recurrence,” notes the researcher, who has been working on the development of CAR-T cells for 15 years.
Robotic system “The case treated in Ribeirão Preto shows that Brazilian science has the capacity to develop highly sophisticated therapies,” comments Kenneth Gollob, who, with hematologist Jayr Schmidt Filho, is working to establish a cell immunotherapy center at A.C.Camargo.
For hematologist Nelson Hamerschlak, from the School of Health Sciences associated with Hospital Israelita Albert Einstein, in São Paulo, it’s the culmination of efforts by a group with extensive experience in cell therapy. At Einstein Hospital, Hamerschlak’s team, and the team of biomedical researcher Luciana Marti, recently created vectors and built DNA sequences that encode fragments of a virus protein (cytomegalovirus) to be inserted into T cells. The procedure should cause the T cells to attack both B cells and cytomegalovirus, which can damage the organs of people who have undergone bone marrow transplants. Instead of assembling a complex structure like that at USP, the Einstein group opted to purchase equipment that produces these cells using automation, which is being tested at US research centers.
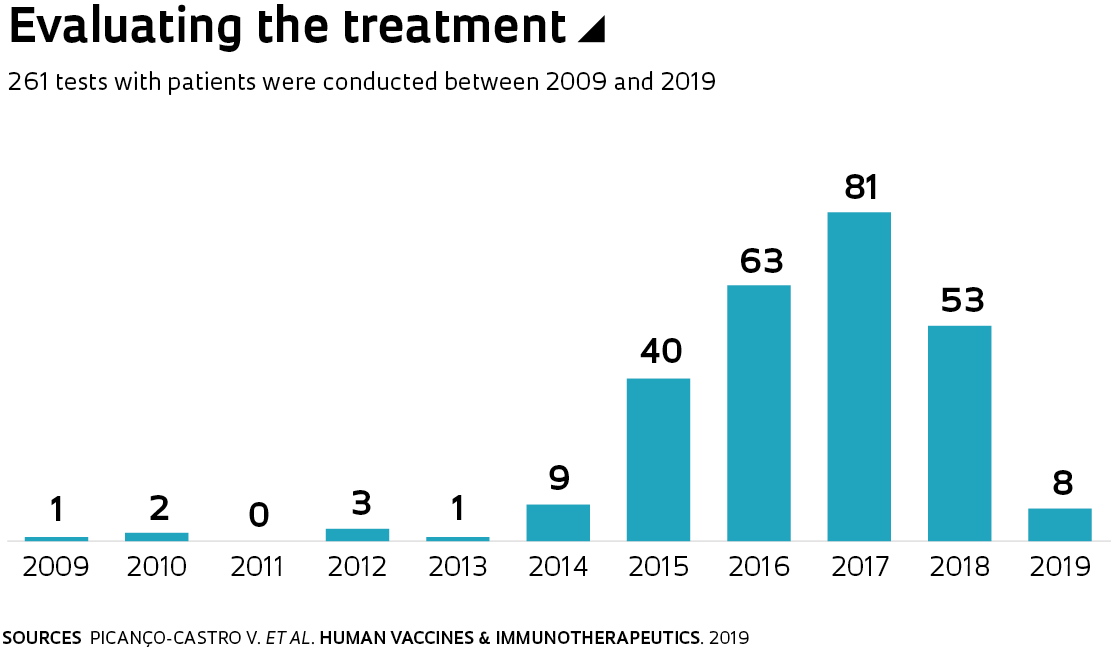
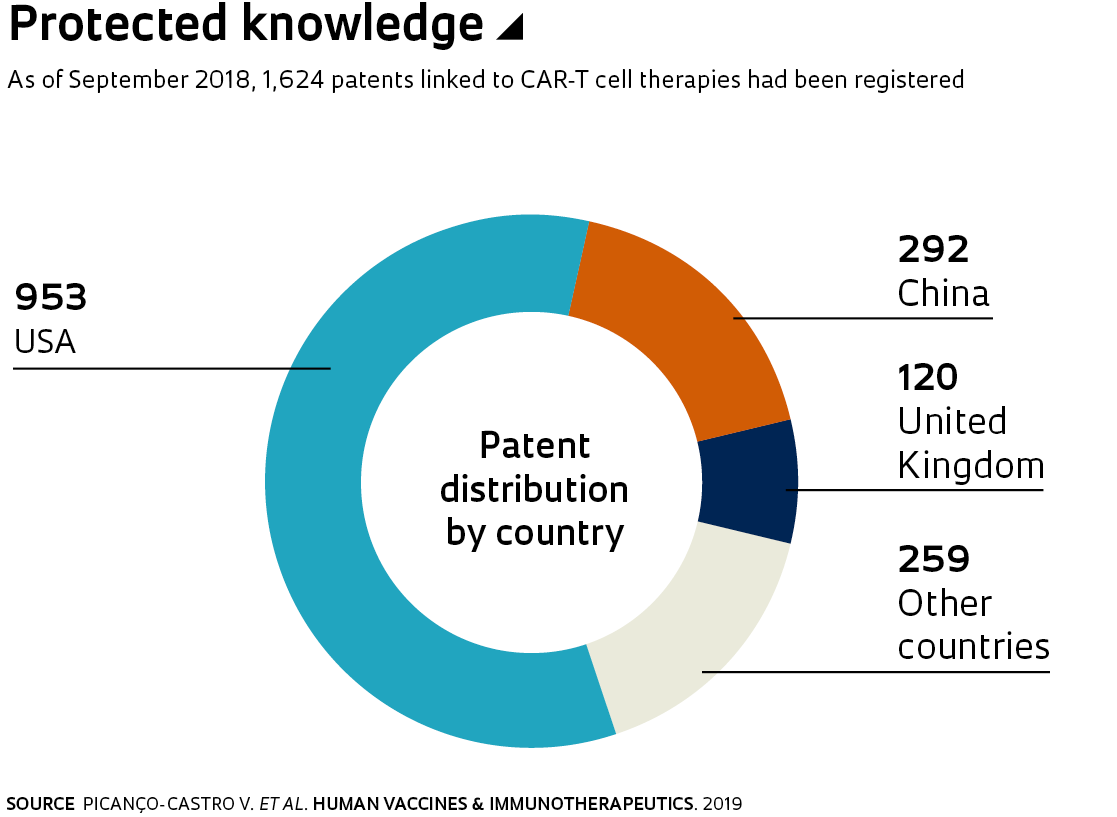
Promising treatment results have led to diversification in CAR-T production techniques and targets. As of September 2018, there were 679 different therapies, with 1,624 patents, according to a survey by the teams of Picanço e Castro and Geciane Porto, a researcher in the field of innovation and entrepreneurship management at the School of Economics, Administration and Accounting at USP-RP. Published in November in Human Vaccines & Immunotherapeutics, the study indicates that an important number of these therapies (218) target B cells, which are associated with hematological tumors. Another 95, however, had been developed—and were in the early stages of testing–to fight solid tumors, which affect the brain, breast, and other organs.
In addition to trying to expand the treatment’s possibilities, various groups are looking for simpler, safer techniques for altering T cells. At INCA, Bonamino’s team is working on a strategy for producing CAR-T cells that doesn’t require viruses. The technique uses fragments of DNA called transposons to insert the desired genes into T cells. Transposons change their position in the genome. Years ago, however, a variety dubbed “sleeping beauty” was developed, which can be applied therapeutically.
Using this strategy, the INCA group produced CAR-T cells that simultaneously fight neoplastic B cells and the Epstein-Barr virus, which can cause leukemia in people with weakened immune systems. These CAR-T cells have been shown to be effective in tests with in vitro cells and in mice with leukemia, according to a study published this April in Human Gene Therapy. In a more recent study, Bonamino and his team showed that it may be possible to skip in vitro multiplication of these CAR-T cells, a step that takes days of preparation and can exhaust them. “We are carefully studying each stage of these protocols before testing them on patients,” the INCA researcher says.
If ongoing studies confirm the efficacy of CAR-T cells against leukemias and lymphomas, the treatment may become an alternative to the use of antibodies, which need to be administered for life, and to bone marrow transplantation, which is more aggressive. Bonamino’s initial calculations indicate that each year, about 900 Brazilians with one of these types of cancer could become candidates for treatment with genetically modified cells.
One challenge will be to make it accessible to more people. “At the moment, each country is looking for a solution,” says Covas. He estimates that Costa’s therapy in Ribeirão Preto ended up costing less than R$100,000. This figure includes hospital and material expenses, in addition to the medical team’s time, and is lower than that of a commercial treatment because it took advantage of the infrastructure available at the university.
In England, for example, the government negotiated with pharmaceutical companies to purchase the treatment for less than the market value, to make it available in the public health system. For Gollob, from A.C.Camargo, prices should fall if the results remain positive and the public demands access to the therapy. “The creation of national platforms allowing the production of CAR-T cells on a large scale could also help to lower the cost,” he contends.
Today the Ribeirão Preto team estimates that it has the capacity to treat two patients every 40 days (he didn’t say if they have already begun treatment on another patient), because production capacity for the cells is still low. “Our group mastered the entire production cycle for these cells. We need to expand production capacity, with a relatively modest investment,” explains Covas. They estimate that around R$10 million will be needed. For now, it’s difficult to calculate the potential savings that the treatment could generate for the public health system (SUS). “The patient we treated had cancer for two years and had undergone four different therapies through SUS,” Covas observes.
Projects 1. Cell Therapy Center (CTC) (nº 13/08135-2); Grant Mechanism Research, Innovation, and Dissemination Centers (RIDC); Principal Investigator Dimas Tadeu Covas (USP); Investment R$45,925,435.79. 2. INCT 2014: On stem cells and cell therapy in cancer (nº 14/50947-7); Grant Mechanism Thematic Project; Principal Investigator Dimas Tadeu Covas (USP); Investment R$3,324,699.34 (CNPq/FAPESP).
This article may be republished online under the CC-BY-NC-ND Creative Commons license. The Pesquisa FAPESP Digital Content Republishing Policy, specified here, must be followed. In summary, the text must not be edited and the author(s) and source (Pesquisa FAPESP) must be credited. Using the HTML button will ensure that these standards are followed. If reproducing only the text, please consult the Digital Republishing Policy.