
LÉO RAMOSMário Bernardes during a training session at InCor: more willingness to perform daily activitiesLÉO RAMOS
Mário Pedro Bernardes is a big, strong man. At a height of over 6 feet, he was used to performing tasks that required physical strength. He had been a cameraman for a TV network for many years and on reporting assignments, he carried a camera weighing 7 kilos on his shoulders. But in 2012, at age 47, he had to retire. Bernardes was given a physical examination prior to participating in a study as a healthy volunteer when he learned that his heart was not working very well. A previous viral infection, probably an old one, had caused lesions in the cardiac muscle and was no longer pumping blood as it should. He had developed heart failure, a complex problem that reduces the heart’s capacity to distribute blood throughout the body and is a major cause of death in Brazil.
A heart attack occurring months later left Mario hospitalized for a week in an ICU and has exacerbated the situation. When discharged, he retired because of his disability and his cardiologist at the time recommended that he not engage in physical activity. He was advised to take drugs to help his heart function and could, at most, take “light walks.” But even that he was unable to do. “After walking a block I had to stop and rest; if I wanted to speak, it was hard,” said Bernardes on a November morning in 2015, shortly after a training session in which he pedaled an exercise bike for 40 minutes at one of the laboratories of the University of São Paulo Heart Institute (InCor-USP).
Bernardes is one of nearly 150 volunteers who in recent years have undergone a training program at the Heart Institute to evaluate the effect of physical exercise on the health of people with heart failure. The program, which is directed by a physiologist, Dr. Carlos Eduardo Negrão, is helping to show that, in addition to the use of drugs, regular physical exercise is essential restoring the health of people with this condition. “Of those who participated in the training, most showed improvement,” says researcher Lígia Antunes-Corrêa, a member of the group.
Only those in a stable clinical condition, obtained with the help of drugs, can participate in the program. Researchers assess the cardiorespiratory capacity of each individual and prepare a progressive training plan so each can reach his or her desired level of physical exercise. The goal is to do 40 minutes of aerobic exercise and another 20 minutes of resistance and flexibility exercises three times a week. The training lasts four months, long enough to begin to recover their former quality of life and ability to perform many daily activities, such as bathing on their own or taking a walk to the supermarket that had been lost with heart failure.
 “After I did the first workout, I felt better,” says Bernardes, who, now at the age of 50, is participating in a second study being conducted by the Negrão group. Much of that good feeling, however, disappeared when Mario stopped doing physical exercise. “The effect of exercise is lost once it is discontinued,” says Antunes-Corrêa.
“After I did the first workout, I felt better,” says Bernardes, who, now at the age of 50, is participating in a second study being conducted by the Negrão group. Much of that good feeling, however, disappeared when Mario stopped doing physical exercise. “The effect of exercise is lost once it is discontinued,” says Antunes-Corrêa.
“Regular physical exercise is essential for people with heart failure with adequate clinical control,” says Negrão, director of the Cardiovascular Rehabilitation and Exercise Physiology Unit of InCor. Since the late 1990s, he and his team have shown that exercise helps to stabilize—and often reverses—the changes that heart failure causes in the body; it functions as a complement to drug treatment.
In these almost 20 years, the work of his group in parallel with the teams in Europe and the United States, has identified some of the changes at the biochemical, cellular and tissue levels induced by exercise. These are changes that rebalance the functioning of muscular, vascular and endocrine systems and help explain how regular physical exercise improves the well-being of people with heart failure.
The evidence accumulated during this period has led to exercise being incorporated into treatment strategies for heart failure, as recommended by the Brazilian Society of Cardiology (SBC), the American College of Cardiology and the American College of Sports Medicine. “Up until the 1990s, there were doubts about the benefits of exercise, and rest was recommended,” says Dirceu Rodrigues de Almeida, SBC’s Chairman of the Department of Heart Failure and head of the Division of Heart Failure and Cardiac Transplantation at the Federal University of São Paulo (Unifesp). Since then, a lot of has changed. “Even in the 1990s evidence began to emerge that physical exercise increased patient well-being, and in the next decade an understanding emerged of how it minimized and even reversed the changes caused by heart failure.”
In the United States, where about 3% of the population have heart failure, most cases arise from a heart attack. In Brazil, where there are about 200,000 new cases each year, the pattern is a little different, as shown in a study conducted by SBC with 1,263 patients treated at 51 centers. In Brazil 30% of cases are the result of a heart attack, 20% from untreated hypertension and 11% from Chagas’ disease, the main cause in Brazil’s Central-West region (see details).
All these events damage the heart muscle—especially the left ventricle, which pushes blood throughout the body—and compromise the heart’s pumping capacity. When blood does not have sufficient force to penetrate the organs and muscles, compensatory mechanisms are immediately triggered. The kidneys release the protein renin into the blood, which triggers a series of chemical reactions culminating in the production of the protein fragment (peptide) angiotensin II. This peptide causes fluid retention in the body and reduces the size of the blood vessels. At the same time, it stimulates the sympathetic nervous system to send commands, increasing the force of contraction and the frequency of heart beats, in addition to further reducing the size of the blood vessels in less vital organs. It is an adaptive mechanism that helps to restore hemodynamic balance.
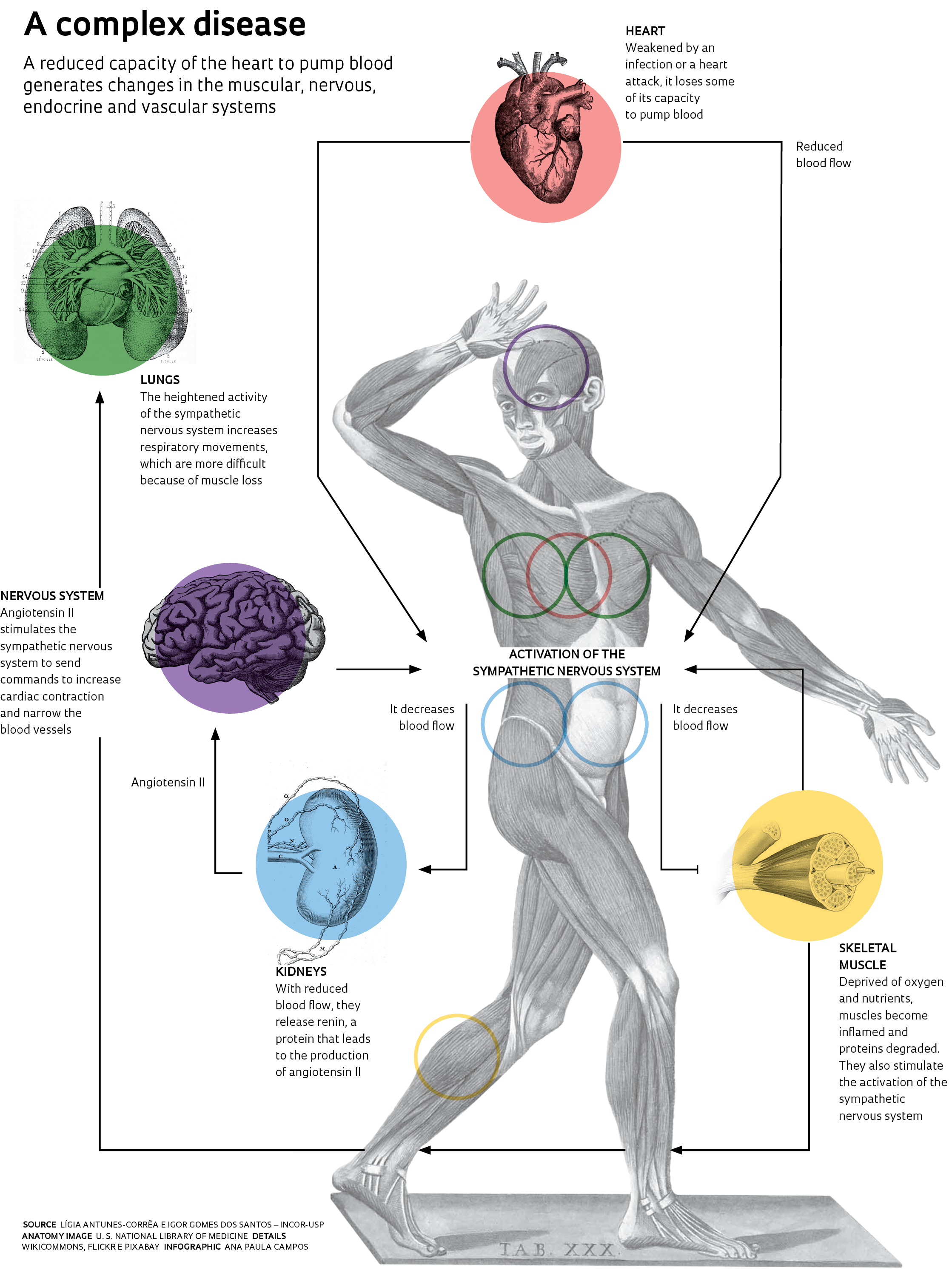 For a time, this effect is good, and even desirable, because it compensates in part for the heart’s lack of strength. It ensures an adequate supply of blood and nutrients to the muscles, for climbing a flight of stairs or performing other daily activities, for example. “But keeping the system activated is costly to the body, not to mention harmful,” notes Igor Lucas Gomes-Santos of the InCor team.
For a time, this effect is good, and even desirable, because it compensates in part for the heart’s lack of strength. It ensures an adequate supply of blood and nutrients to the muscles, for climbing a flight of stairs or performing other daily activities, for example. “But keeping the system activated is costly to the body, not to mention harmful,” notes Igor Lucas Gomes-Santos of the InCor team.
This effort causes anatomical and functional changes in the diseased heart. It becomes more spherical and pumps blood even less efficiently. Another problem is the severe loss of muscle mass (cachexia). Almost half of those with congestive heart failure lose weight because their muscles begin to waste away, which is the reason for the weakness and tiredness they feel.
The excess of angiotensin II in the bloodstream and the activated sympathetic nervous system, which are continuously stimulating the blood vessels to remain at a reduced size (vasoconstriction), end up modifying the oxygen and nutrient (glucose) supply to the muscle cells. These cells circumvent the problem by triggering an alternative source of energy production. The cells begin to consume their own proteins, in a series of chemical reactions that do not rely on oxygen and lead to the accumulation of lactic acid, the same compound responsible for muscle soreness after an intense physical workout. “These people live with the feeling of constant physical exhaustion,” says Dr. Maria Janieire Alves, a cardiologist and member of the Negrão team. “Some of them feel tired and short of breath from just combing their hair,” says Antunes-Corrêa.
And that’s not all. In addition to using proteins to generate energy, the muscles have another imbalance, which was discovered in 2012 by a research team working for Patrícia Chakur Brum, a Negrão collaborator. In her laboratory at the School of Physical Education and Sports (EEFE-USP), she and researchers Aline Villa Nova Bacurau and Telma Cunha analyzed how the skeletal muscle cells of rodents and humans with heart failure functioned. They found that in both cases, the more degraded the cells were, the more they synthesized proteins, leading to muscle atrophy. With further research, Brum noted increased inflammation and the production of reactive oxygen species, molecules that damage muscle proteins. A quality control system identifies defective proteins and sends them to a disassembly line, contributing to the loss of muscle mass.
In 2012, Júlio Cesar Ferreira, a former PhD student of Brum and now a professor at USP’s Institute of Biomedical Sciences (ICB/USP), also found that there were problems with the quality control of the heart muscle proteins. He analyzed the heart cells of rodents and humans who had undergone surgery to replace heart valves, and found that the proteins they produced were of poor quality and compromised organ contraction capacity.
Brum and two researchers under her supervision for their doctorates—Alessandra Medeiros, of Unifesp located in Baixada Santista (São Paulo State) and Natale Rolim, the Norwegian University of Science and Technology—showed that aerobic physical exercise could reverse the changes in heart muscle function. For two months, they had rodents with heart failure run on a treadmill for one hour a day, five times a week. After the training, the heart cells showed improvement in the quality control of proteins, and the heart contractions began to recover. Protein degradation decreased in the skeletal muscles. “Exercise improves fitness by improving the functioning of the heart and skeletal muscles,” says Brum.
 Regular physical exercise also undoes the imbalance caused by angiotensin II in the muscles. Rodents subjected to the treadmill training regimen produce compounds in their muscle cells that transform angiotensin II into a smaller molecule: angiotensin 1-7. This version of angiotensin causes the blood vessels to dilate and reduces cardiac remodeling. “The effects of exercise complement drug treatment, but they are unable, for example, to completely or permanently inhibit the action of angiotensin II,” says Gomes-Santos.
Regular physical exercise also undoes the imbalance caused by angiotensin II in the muscles. Rodents subjected to the treadmill training regimen produce compounds in their muscle cells that transform angiotensin II into a smaller molecule: angiotensin 1-7. This version of angiotensin causes the blood vessels to dilate and reduces cardiac remodeling. “The effects of exercise complement drug treatment, but they are unable, for example, to completely or permanently inhibit the action of angiotensin II,” says Gomes-Santos.
Exercise also restores blood flow in the muscles by reducing the activity of the sympathetic nervous system. In a study of 26 people with heart failure, Antunes-Corrêa compared the sympathetic nervous system functioning of 13 who exercised for one hour a day three times a week for four months with the other 13 who received only a recommendation to maintain their regular lifestyle. She found that exercise restored the functioning of cells that detect motion (mechanoreceptors) and chemical compounds (chemical receptors) located in the muscles and near the blood vessels. These receptors control the activation of the sympathetic nervous system during muscle contractions and are deregulated in heart failure. As a result of exercise, people’s hearts beat more slowly and respiration required less effort during physical exertion. “Exercise seemed to normalize everything that was changed,” says Gomes-Santos.
Despite favorable evidence of its benefit, regular exercise is still far from being part of the lives of those with heart failure, according to Dirceu de Almeida of the Cardiology Society (SBC). Three factors contribute to this: many doctors are still unaware of the benefits of exercise and recommend that the patient rest; lack of cardiovascular rehabilitation centers in Brazilian hospitals; and patients who are unaware of the severity of the condition.
“Before treating heart failure through the use of beta blockers, which reduce sympathetic nervous system activity, the average life expectancy was one year after diagnosis. These patients now live up to 10 years,” says Alves. “The challenge with training is to improve the quality of their lives and reduce heart decompensation.” She followed a group of people with advanced heart failure who did physical activity for one year and were then instructed to remain active. Only 40% continued to exercise. “In the group that continued to exercise, 10% died,” she says. In the group that did not continue to engage in exercise, mortality was 50%.
Projects
1. Cellular and functional bases of physical exercise in cardiovascular disease (nº 2010/50048-1); Grant Mechanism Thematic Project; Principal Investigator Carlos Eduardo Negrão (InCor-USP); Investment R$2,428,870.57 (for the entire project).
2. Effects of aerobic physical training associated with inspiratory muscle training on skeletal myopathy in patients with heart failure (nº 2013/15651-7); Grant Mechanism Scholarships in Brazil – Postdoctoral; Principal Investigator Carlos Eduardo Negrão (InCor-USP); Recipient Lígia de Moraes Antunes-Corrêa (InCor-USP); Investment R$150,763.78.
3. Contribution of myogenic precursor cells in skeletal myopathy induced by heart failure: therapeutic perspective of aerobic exercise training (nº 2014/23703-0); Grant Mechanism Regular Research Grant; Principal investigator Patrícia Chakur Brum (EEFE-USP); Investment R$369,007.10.
Scientific articles
NEGRÃO, C. E. et al. Effects of exercise training on neurovascular control and skeletal myopathy in systolic heart failure. American Journal of Physiology – Heart and Circulatory Physiology. V. 308, pp. H792-H802. February 2015.
ALBUQUERQUE, D.C. et al. I Brazilian registry of heart failure – Clinical aspects, care quality and hospitalization outcomes. Arquivos Brasileiros de Cardiologia. V.104 (6), pp. 433-42. June 2015.
CUNHA, T.F. et al. Exercise training prevents oxidative stress and ubiquitin-proteasome system overactivity and reverse skeletal muscle atrophy in heart failure. PLOS One. August 3, 2012.
CAMPOS, J.C. et al. Exercise training restores cardiac protein quality control in heart failure. PLOS One. December 27, 2012.
GROEHS, R. et al. Exercise training prevents the deterioration in the arterial baroreflex control of sympathetic nerve activity in chronic heart failure patients. American Journal of Physiology – Heart and Circulatory Physiology. V. 308 (9), pp. H1096-H1102. May 1, 2015.