
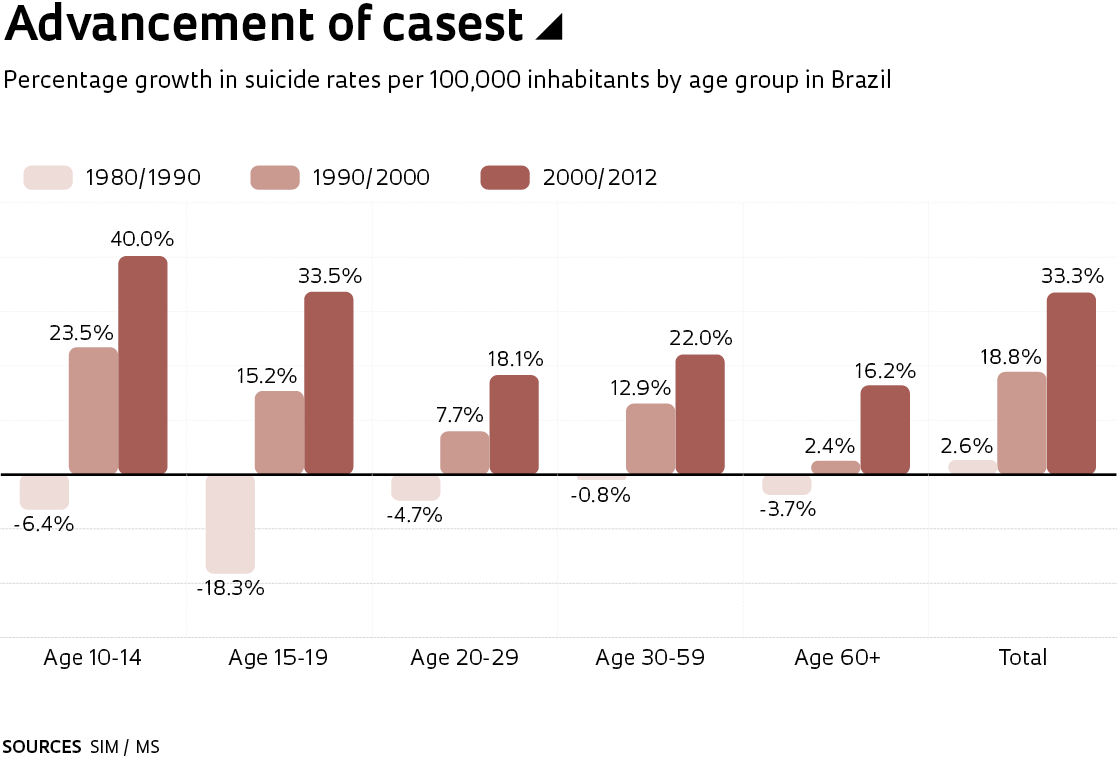
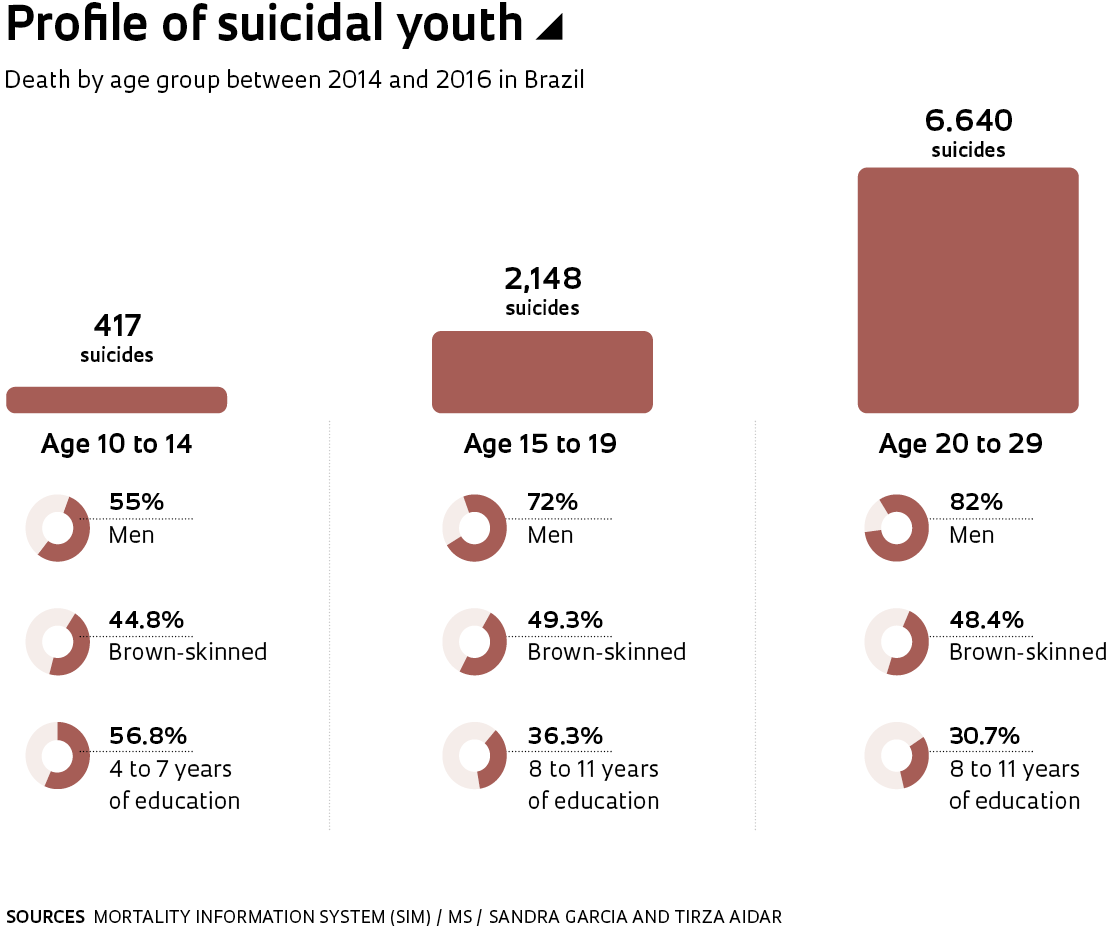
Between 2000 and 2012, 49.4% of the 172 countries in the World Health Organization (WHO) have recorded decreases greater than 10% in suicide rates. On the other hand, Brazil had an increase of 10.4%, with significant growth among the younger population. More recent statistics from the Brazilian Ministry of Health indicate that self-inflicted deaths in the age range of 10 to 14 have increased 40% among boys and 30% among girls, between 1997 and 2015. “Psychic conflicts, alcohol and drug abuse, violent displays, in addition to gaps in integrated public policy to prevent suicidal behavior, are some of the hypotheses for this situation,” says anthropologist Sandra Garcia, coordinator of the Brazilian Center for Analysis and Planning (CEBRAP), which has researched the phenomenon in Brazil since last year.
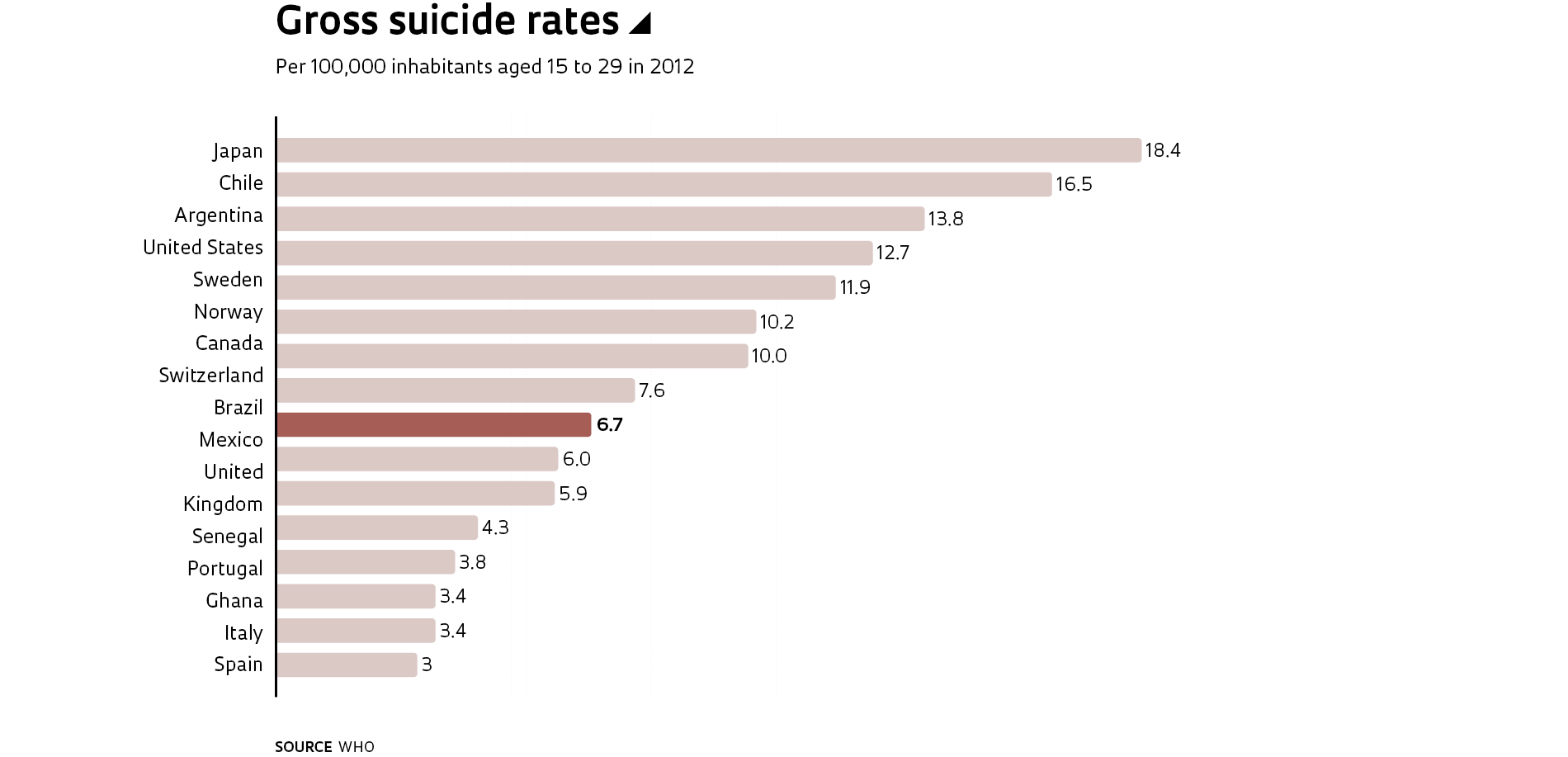
Every year one million suicides are registered worldwide and, for each death, says Garcia, there are at least 20 unsuccessful attempts. Based on the data analysis by the Ministry of Health, researchers at CEBRAP and the “Elza Berquó” Population Studies Center (NEPO) at the University of Campinas (CAMPINAS) identified that, in Brazil, suicide was the fourth cause of death among individuals 15 to 29 years old, between 2011 and 2016, with numbers nearly four times higher among men (9 deaths per 100,000 inhabitants) in relation to women (2.4 deaths per 100,000 inhabitants). With the exception of the 15 to 19 age group in the Central-West, in all other regions of Brazil women attempt to end their life more than men. “Among girls aged 10 to 14 in the Northeast, the incidence of self-mutilation reaches 39.7%,” informs Garcia.
The researcher also calls attention to the increase among indigenous people. “Among this population, the proportion of deaths by suicide for every 100,000 inhabitants is 12, double the national average [5.7],” she says. According to the researcher, historically, the southern region of Brazil registers the highest number of suicides, with 12 deaths per 100,000 inhabitants per year. “Ten years ago, in the northern region of Brazil, this figure was 7. Now this figure also reached 12 suicides per 100,000 inhabitants, growth that was motivated by an increase in indigenous suicide,” she believes. In relation to the global situation, the anthropologist notes that, in countries of higher income, mortality by suicide is 3.5 times higher among men. On the other hand, the incidence of suicidal thoughts is higher among women. Despite the growth trend, in Brazil the prevalence of suicide continues to be underestimated due to lower registry of cases or errors in classification. According to Garcia, some deaths are considered “accidental” or registered as “undetermined cause,” either because of notification errors or even by omission by the family itself.
Responsible for establishing this new line of investigation at CEBRAP, demographer Elza Berquó, professor emeritus at the School of Public Health at the University of São Paulo (FSP-USP), says that she decided to include the topic of suicide in demographic studies after identifying two phenomena: the increase in young people testing HIV positive and the rise in cases of unwanted pregnancy. “Why do these phenomena occur at a time when adolescents can prevent them using, for example, condoms or the morning after pill?” she asks. In her search for answers, Berquó hypothesized that young people want to run risks as a way to find meaning for their lives.
Mental health
It has been estimated that more than 90% of suicide cases are linked to the presence of some sort of mental disorder, including depression, bipolar disorder, and schizophrenia. A study developed by researchers from the American institutions San Diego State University, Florida State University, Lynn University, and Pomona College analyzed the incidence of mental disorders and cases of suicide in adolescents and adults in the United States. The research identified that, between 2005 and 2017, the rates of depression increased 52% among adolescents 12 to 17 years of age and, from 2009 to 2017, rose 63% among adults aged 18 to 25. In this age range, the same study claimed that, between 2008 and 2017, there was an increase of 71% in the registrations of serious psychological suffering. Such growth tendencies are weak or nonexistent in adults over 26 years, which indicates a generational change in the incidence of mental disorders. The study suggests that the increase in psychological suffering among the younger population could be related to the use of electronic devices and social media, in addition to a reduction in sleep.
“In Brazil, we have identified that depression affects younger people, who are becoming more and more solitary and seekers of immediate gratification. It is a generation that turns to self-mutilation as a form of expressing pain,” confirms psychiatrist Neury José Botega, of the School of Medical Sciences (FCM-UNICAMP). Guilherme Vanoni Polanczyk, of the Department of Psychiatry at the USP School of Medicine (FM-USP), explains that, in some cases, mental disorders that are not treated, or are inappropriately treated, can lead to suicide.

Aware of this situation, researchers at the Institute of Psychiatry (IPq) at FM-USP, the Federal University of São Paulo (UNIFESP), and the Federal University of Rio Grande do Sul (UFRGS), who are part of the Brazilian Psychiatric Institute for Development (INPD), analyzed the development of 2,511 children from 6 to 12 years registered in public schools in Porto Alegre and São Paulo and identified 651 with some kind of mental disorder, such as anxiety, phobias, attention deficit, hyperactivity, and schizophrenia. “Of these children, 81% had never received psychiatric or psychological treatment. We also verified that brown children have a greater chance of not being treated, in comparison with white children,” states psychologist Daniel Fatori, postdoctoral student at IPq and one of the authors of the study.
Polanczyk explains that close to 14% of children and adolescents worldwide have some type of mental disorder. “In developed countries, close to 35% of children with these disorders receive treatment, but in Brazil, this falls to about 18%,” he reports. His opinion is that mental disorders arise from a combination of genetic, biological, and environmental factors. “As of yet, there is no cure,” he says. On the other hand, there are an increasing number of studies that seek to develop preventive strategies, as recognition and early intervention guarantee better results for clinical conditions. “Damage to the mother-child bond, for example, in cases of postpartum depression, abandonment, and violence, creates high-risk situations for mental disorders to manifest throughout a lifetime,” he reports.
The project, supervised by Polanczyk, involves identification of pregnant adolescents who live in situations of extreme poverty in São Paulo. “We monitor these young girls from the first trimester through to the baby completing 2 years of age, developing strategies to improve the affective links and avoiding situations of abuse and violence,” explains the researcher, remembering that 75% of adults with mental disorders exhibited the first symptoms before 18 years of age. Polanczyk recalls further that child and adolescent psychiatry represents a new scientific field, with the first studies carried out by European universities as recent as the 1960s. In Brazil, family doctors and pediatricians have limited training in mental health issues affecting children and adolescents. For example, there are very few who know how to assess the occurrence of suicidal thoughts.
Sandra Garcia points out a further difficulty that involves Decree No. 104 of the Ministry of Health. Published in January 2011, it stipulates that municipal medical authorities are obligated to announce all registered suicide attempts and cases. Despite the initiative having fostered improved control of the incidence of self-inflicted violence, its registration form is flawed. For example, it does not include information about previous attempts. “The history of previous attempts represents the most important indicator of suicide. The form should require this information,” she notes.
A survey carried out by the Regional Center for Studies on the Development of the Information Society (CETIC) shows that 85% of children and adolescents between 9 and 17 years of age in Brazil used the internet in 2017, which equates to 24.7 million people. “Close to 80% of these users navigate the web every day. While they are totally connected, they can be isolated. In other words, if they are experiencing depression or anguish, when they disconnect, they may not find adequate support, which tends to accentuate the suffering,” according to the anthropologist from CEBRAP. Despite the lack of studies that prove the direct relationship between the abusive use of technology and the appearance of symptoms of depression or anxiety, Polanczyk considers it necessary to evaluate not only the number of hours that youth spend in front of computer screens, tablets, and cell phones, but also the content accessed. “The question we must ask is: who uses what content? An adolescent with symptoms of depression who, for example, has social difficulties, may look to the internet for situations that reflect or strengthen his or her emotional state via sites that encourage self-harm or even suicide,” warns the psychiatrist.
Vulnerable population
The socioeconomic situation of the country is another factor that can be related to the increase in suicide. According to the Continuous National Household Sample Survey: Education (Continuous PNAD) published in 2017, 23% of Brazilian youth from 15 to 29 years—that is, 11.2 million out of 48.5 million—did not study or work in 2016. Between 2016 and 2017, there was an increase of 5.9% in this age group, with the majority being poor and having little education, and two-thirds being women and half of them with children. Besides this, 41% of Brazilian youth abandon high school before completion, according to data from the Brazilian Institute of Geography and Statistics (IBGE). “Young people outside the education system and labor market, and who are subject to economic and social vulnerability, are more exposed to mental problems and to abuse of licit and illicit drugs,” notes Garcia of CEBRAP.
Aware of the socioeconomic fluctuations that occurred in Brazil between 2006 and 2015, research developed by UNIFESP also identified the correlation between unemployment, economic crisis, and suicide. One of the authors of the study, psychiatrist Elson Asevedo, of the Paulista School of Medicine, says that the study recognized the vulnerability of the population aged 15 to 19. “We observed that, in moments of economic crisis, suicides increase in this age group,” he informs, explaining that, in addition to the Ministry of Health, the research works with information about per capita Gross Domestic Product (GDP), unemployment tax, and the Gini coefficient, which measures inequality. Another finding involves the growth of suicide in capital cities. “While suicide in adolescents increased 13% in Brazil, in the capitals, the corresponding increase was 24%,” he says. “In the big cities, people are more exposed to risk factors for mental disorder, such as violence, and they tend to have fewer social bonds.”
SOCIODEMOGRAPHIC
Unemployment
Migration
Social isolation
Wars and armed conflict
PSYCHOLOGICAL
Interpersonal conflict
Loss of family members or friends
Political and financial changes
Discrimination
CLINICAL CONDITIONS
Mental disorders
Depression and change of mood
Alcoholism
Chronic pain and serious injury
SOURCE MS
Paths to prevention
Some universities have created programs to deal with this situation. USP, which last year recorded only four cases of suicide involving its students, established the Office for Mental Health in July. “Through contact with family members, friends, and professors of the students who took their own life, we observed that each act had a distinct motivation. Two cases involved young people who exhibited some type of mental disorder and seemed to be having difficulty dealing with frustration, but another surprised the entire family and school community,” says Andrés Eduardo Aguirre Antúnez, vice director of the Institute of Psychology at USP and coordinator of the office. “We must be attentive to people who walk alone much of the time and who verbalize that life is not worth living. Suicide can happen on an impulse and in situations that are even a mystery for the most experienced clinician,” he says. The majority of the 115 students who have passed through the office in its first six months of operation reported suffering from situations of violence or family abandonment, reports Antúnez. All who were in agreement were sent for care at the university’s Institute of Psychology or Institute of Psychiatry. “In addition to treating these young people, we are producing knowledge. Today, there are four doctoral and postdoctoral studies underway, based on the cases that come to the office,” he informs.
With regard to public policy for the reduction of suicide rates, Neury Botega, of UNICAMP, recalls that, in order to be effective, they must consider the unique features of each country from a historical, social, and economic perspective. According to Botega, in countries such as China and India, where suicide rates are high among women, the percentages dropped as the urbanization process settled. “In cities with more freedom, the social role of women began to change. Many began to live with greater autonomy in relation to their husbands,” he says. Countries such as Austria and Australia, which registered high rates of self-inflicted death by firearm, put into action disarmament campaigns, while the United Kingdom, with high percentage rates of suicide among the elderly, created a project to care for the population over 60 years of age. “In Russia, the reduction in suicide is linked to laws that restrict the use of alcohol, and in Sweden, which in the 2000s faced an economic recession, the strategy involved a support program for the unemployed,” compares the researcher from UNICAMP.
In Brazil, policies for suicide prevention are primarily the domain of the Ministry of Health, including Decree No. 104 of 2011, and awareness campaigns. Until recently, the country did not have nationwide legislation, a situation that changed at the end of April with the enactment of Law No. 13.819/19, which instituted the National Policy for the Prevention of Self-mutilation and Suicide. From this point forward, public and private schools are obligated to notify guardianship agencies about cases of self-inflicted violence, even if they are not confirmed. For Sandra Garcia, of CEBRAP, such a requirement could be harmful in situations where a child’s suffering is associated with abuse by family members, since the guardianship agency must alert those responsible whenever they are notified. “The schools must work together with the health services to take care of these youth,” she says. Asevedo, of UNIFESP, sees the new law as positive. “It makes the issue a priority on the government agenda and fosters the development of integrated public policies,” he concludes.
Project
Interventions in early childhood and trajectories of cognitive, social, and emotional development (no. 16/22455-8); Grant Mechanism Thematic Project; Principal Investigator Guilherme Vanoni Polanczyk (USP); Investment R$3,175,305.64.
Scientific articles
FATORI, D. et al. Use of mental health services by children with mental disorders in two major cities in Brazil. Psychiatric Services. Vol. 70, no. 4, pp.337–41. Apr. 1, 2019.
TWENGE, J. M. et al. Age, period, and cohort trends in mood disorder indicators and suicide related outcomes in a nationally representative dataset, 2005–2017. Journal of Abnormal Psychology. Vol. 128, no. 3, pp. 185–99. Apr. 2019.
JAEN-VARAS, D. et al. The association between adolescent suicide rates and socioeconomic indicators in Brazil: a 10-year retrospective ecological study. Brazilian Journal of Psychiatry. Online. Feb. 18, 2019.