

Elizabeth di Lullo
Zika in the mini-brain: AXL receptor (green), potential key to how the virus penetrates the precursor cells (red) of brain tissueunitElizabeth di LulloIn late March 2016, the World Health Organization (WHO) changed its position on the connection between the Zika virus and recent cases of microcephaly and other neurological problems. In a report released on March 31, 2016, it said that there was a “strong scientific consensus” that the Zika virus causes microcephaly, a condition in which infants are born with heads that are too small in relation to the gestation period, and Guillain-Barré syndrome, a degeneration of the myelin sheath of the nerves that can cause paralysis. It is an important shift in position, adopted two months after considering that there was a “potential association” between the virus and these problems and declaring a public health emergency international in scope.
Recognition of the so-named causality relationship results from the accumulation of two types of evidence. The first type is epidemiological. Since it was identified in Brazil in 2015, the virus has spread to 32 other countries in the Americas (although not necessarily from Brazil), plus some countries in Asia, Europe and Africa—in six countries the transmission seems to be exclusively sexual. Added to this is the rise in the number of microcephaly cases associated with the Zika infection, which has already been found in eight countries. As of March 26, 2016, Brazil had the largest number of babies (944) with microcephaly—the virus was detected in 130 of them. Colombia and French Polynesia had the second highest number, each with eight cases.
The second type of evidence is biological. Since the Zika virus gained international attention in November 2016, the number of scientific papers on Zika has increased exponentially. PubMed, a database of articles in the biomedical field, listed 218 works between 1952 and 2015. There have been 307 in 2016 alone. The cause of the increase is the coalescing of researchers from different disciplines and countries around a common problem. “Rarely have scientists become so engaged in a new research agenda with such a sense of urgency,” wrote the Brazilian epidemiologist Laura Rodrigues of the London School of Hygiene & Tropical Medicine, in a commentary on the subject in The Lancet.
One of the studies that was instrumental in changing the view of the scientific community about the causality of microcephaly was conducted by Slovenian researchers. The group led by virologist Tatjana Avsic-Zupanc of the University of Ljubljana, found the virus and quantified its presence in the brain of an eight-month-old baby with microcephaly. The child’s mother had lived in Natal, in Rio Grande do Norte State, where she became pregnant in February 2015. Three months later she showed signs of Zika infection—fever, rash, itching, muscle and eye pain. The third ultrasound examination, done at 29 weeks of gestation, identified the baby’s growth restriction and reduced skull size. In addition to microcephaly, the researchers observed lesions (calcifications) in the brain. Published in February 2016 in the New England Journal of Medicine, the work was considered one of the first solid pieces of evidence that the virus and microcephaly were connected, although Brazilian virologist Pedro Vasconcelos of the Evandro Chagas Institute, in Pará State, had already isolated the virus from the brain and other tissues of a baby from the state of Ceará with microcephaly (see Pesquisa FAPESP Issue nº 239).
Since then, other studies have accumulated evidence that the Zika virus is able to cross the placenta and infect the amniotic fluid, something that few viruses can do. The presence of the virus in different tissues is not enough to confirm causality however. It could be there without causing damage. Two studies presented in early March 2016 showed that Zika is capable of infecting human neural cells and killing them. In one study, deposited on March 2 in the Peer J Preprints repository, researchers from Rio de Janeiro and São Paulo found that Zika invades and kills the precursor stem cells of neural cells.
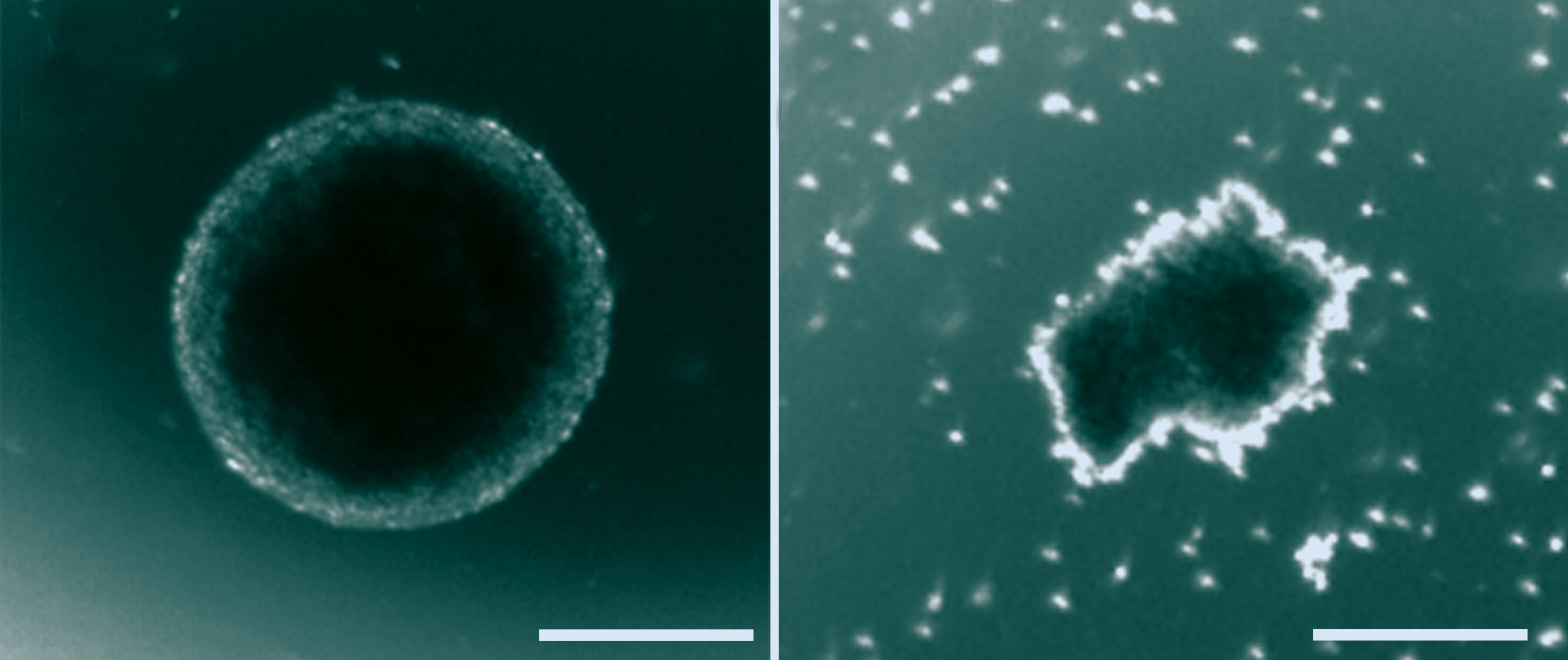
Patricia Garcez/UFRJ and IDOR
Devastating effect: healthy neurospheres (left) and neurospheres generated from cells infected by the Zika virusPatricia Garcez/UFRJ and IDORThe group coordinated by Stevens Rehen and Patrícia Garcez, neuroscientists at the Federal University of Rio de Janeiro (UFRJ) and the D’Or Institute for Research and Education (IDOR), chemically induced skin cells to become pluripotent stem cells, capable of producing various tissues, and then stimulating them to turn into brain cells. Under the right conditions, these cells organize themselves into layers and generate neurospheres and brain organoids (mini-brains), models of the brain at different stages of development. The first cells mimic the brain of an embryo in a rudimentary stage; while mini-brains are equivalent to the brain of a fetus at 3 months.
In the laboratory, the researchers infected stem cells with samples of the African Zika strain, isolated in 1947 and apparently distinct from the one now circulating in Brazil, and analyzed how they developed compared to cells that had not been exposed to the virus. After three days, Rehen and his team observed that the Zika virus had compromised the ability of stem cells to generate neurospheres. “The few neurospheres formed degraded within six days, while those originating from uninfected cells developed normally,” says Rehen.
Electron microscopy images showed that the virus had multiplied rapidly within the cells and had triggered programmed cell death (apoptosis). And the infected mini-brains were 40% smaller than the healthy ones 11 days after the start of testing. In addition to growing less, they were also deformed.
In an extended version of the study, published in April 2016 in Science, the Rio de Janeiro group infected stem cells with the dengue virus, which is genetically very similar to the Zika virus and also widespread in Brazil. The virus invaded the neural progenitor cells more effectively than Zika, but caused no problems. “Unlike Zika, the dengue virus did not affect the development of neurospheres and organoids,” says Rehen.
Two days after the Rio de Janeiro group deposited the work in the Peer J Preprints, U.S. researchers presented confirmation of Zika’s affinity for brain tissue cells in the journal Cell Stem Cell. They put precursor stem cells of neural cells in contact with the virus and found that, three days later, 85% of them were infected and had activated the biochemical pathways of apoptosis. The experiment was repeated with immature kidney cells, and the virus invaded just over 10% of them, indicating a preference for cells of the nervous system. “We showed that the Zika virus infects in vitro neural cells that correspond to those forming the cortex,” said neuroscientist Hongjun Song of Johns Hopkins University, in a press release.

Kuhn and Rossmann research group/Purdue University
Dengue look-alike: frozen copies of the Zika virus…Kuhn and Rossmann research group/Purdue UniversityResearchers of the Zika Virus Research Network in São Paulo (Zika Network), supported by FAPESP, obtained similar evidence. Besides the African Zika virus, they also used the Brazilian strain to infect precursor stem cells of neural cells, neurospheres, mini-brains and pregnant female mice. According to the authors, the results submitted for publication confirm that the virus causes microcephaly.
Causality criteria
“Generally speaking, the Hill criteria is being used to demonstrate that a virus causes a disease,” says virologist Paolo Zanotto, of the University of São Paulo (USP). Proposed in 1965 by the British epidemiologist Austin Bradford Hill, these criteria consist of a list of nine characteristics that in general must be met. They are: strength or effect of size (the stronger the association, the more likely the causal probability); consistency (similar observations made by different groups in different locations increases the probability that the effect exists); specificity (the greater the association between a factor and its effect, the greater the probability of a causal relation); temporality (the effect must occur after exposure to the factor that causes it); biological gradient (the longer the exposure to the causative factor, the greater the effect); plausibility (existence of biological mechanism that explains the relationship between cause and effect); consistency (the connection between laboratory and epidemiological findings increases the probability factor causing the effect); experiment (occasionally can seek experimental evidence); analogy (consideration of alternative explanations).
Despite these advances, no one knows for sure how the virus, once inside the fetus, reaches the brain tissue. Arnold Kriegstein and his group at the University of California at San Francisco suspect that the virus reaches the nervous system through the fluid that bathes the central nervous system (cerebrospinal fluid) and uses the AXL receptor expressed in the precursor brain cells to invade them (a detailed explanation appears in the online text).
The most significant confirmation that the Zika virus causes microcephaly comes from studies such as the one done by infectious disease specialist Patrícia Brasil of Fiocruz in Rio de Janeiro. Since September 2015, she has been following pregnant women who showed signs of the Zika infection at different stages of pregnancy. In March 2016, Brasil presented her initial findings in the New England Journal of Medicine. The researchers identified the virus in 72 of the 88 participants—only 42 continued in the study and agreed to imaging tests on the infants. Of the 42 infants, 12 (29% of the total) had various degrees of compromise: from intrauterine growth restriction (five cases) to brain lesions (seven) and fetal death (two)—some had more than one problem.
Risk in the first trimester
More evidence of causality came from a study that retrospectively analyzed the Zika outbreak in French Polynesia. Simon Cauchemez of the Pasteur Institute in Paris, estimated the total number of cases of the infection based on serological test data. In a search of medical records, he and his colleagues identified eight cases of microcephaly between September 2013 and July 2015. Using a mathematical model, they concluded that an infection in the first trimester of pregnancy is the one that most increases the probability of having a baby with microcephaly. According to the results, reported in The Lancet, this risk is 1%.

Kuhn and Rossmann research group/Purdue University
…used to determine its detailed structureKuhn and Rossmann research group/Purdue UniversityThe studies measure different phenomena and can not be compared. But they seem sufficient to prove causality. “It’s premature to calculate the amount of risk of an infection leading to the birth of a microcephalic baby based on the Rio de Janeiro and Polynesia study data, since the number of people studied is small,” says epidemiologist Cesar Victora, of the Federal University of Pelotas (UFPel). “As to the causal relationship, there is no doubt,” he says.
“Both works are important, but do not exhaust the subject,” says USP’s Zanotto. “We still need to know if the risk depends on pre-exposure to other pathogens, the prior existence of other diseases, genetic characteristics and the nutritional status of the mother,” he says. Zanotto coordinates the Zika Network, which has developed a test that can identify blood antibodies against the virus.
Although unable to estimate the level of risk of a pregnant Brazilian woman with Zika having a baby with microcephaly, the Fiocruz data go beyond confirming causality. The work reinforces the idea that Zika causes not only microcephaly, but also a congenital syndrome, as some have suggested. In this syndrome, the type of problem presented by the baby depends on what point during the pregnancy the infection occurred. “Once the pregnant woman has been diagnosed with the Zika virus,” says Brasil, “the obstetrician should monitor the baby by conducting tests at shorter intervals.” That was how her group identified in time a case in which the amniotic fluid had dried. The baby was saved by a surgical delivery.
Scientific articles
MLAKAR, J. et al. Zika virus associated with microcephaly. New England Journal of Medicine. February 10, 2016.
GARCEZ, P.P. et al. Zika virus impairs growth in human neurospheres and brain organoids. Peer J Preprints.
TANG, H. et al. Zika virus infects human neural cortical progenitors and attenuates their growth. Cell Stem Cell. May 2016.
SIROHI, D. et al. The 3.8 Å resolution cryo-EM structure of zika virus. Science. March 31, 2016.
BRASIL, P. et al. Zika virus infection in pregnant women in Rio de Janeiro – preliminary report. New England Journal of Medicine. March 4, 2016.
CAUCHEMEZ, S. et al. Association between zika virus and microcephaly in French Polynesia, 2013-15: a retrospective study. The Lancet. March 15, 2016.