
 Larissa RibeiroEverybody is a universe. Literally. An estimated 75 trillion cells and ten times as many bacteria, most of which (100 trillion) can be found in the intestines, make up each and every human body. Although it is not new, this information only began to attract the interest of scientists and the medical field recently. For many years, it was believed that the cohabitation with the microscopic tenants was generally beneficial for the hosts. Or, at least, that it is not preferential or harmful for either of the involved parties. In recent years, however, this idea of peaceful coexistence began to change as studies surfaced showing that this continuous and inevitable intimacy may bring about undesirable consequences for the host.
Larissa RibeiroEverybody is a universe. Literally. An estimated 75 trillion cells and ten times as many bacteria, most of which (100 trillion) can be found in the intestines, make up each and every human body. Although it is not new, this information only began to attract the interest of scientists and the medical field recently. For many years, it was believed that the cohabitation with the microscopic tenants was generally beneficial for the hosts. Or, at least, that it is not preferential or harmful for either of the involved parties. In recent years, however, this idea of peaceful coexistence began to change as studies surfaced showing that this continuous and inevitable intimacy may bring about undesirable consequences for the host.
One such study by Brazilian researchers, published in PLoS Biology in December last year, shows a condition in which intestinal bacteria may harm the human body. With 11 thousand downloads in the few months since publication, it is getting a lot of attention. Physician Mário Abdalla Saad from the State University of Campinas (Unicamp) and his team demonstrated that a certain group of intestinal bacteria may, in some situations, set off a metabolism imbalance. The latter, in turn, almost inevitably leads to diabetes and obesity, which in the last 20 to 30 years have become a major public health issue around the world, affecting 350 and 500 million people, respectively.
The changes that take place prior to diabetes and the excessive weight gain are referred to by the physicians as insulin resistance. The hormone enables muscle cells and other types of tissue to absorb sugar (glucose) from the blood stream and to convert it into energy or store it for future use. When insulin resistance is in place, the body ceases to use this correctly. In their tests on rodents, Saad and his team found that the Firmicutes, a bacteria group made up of dozens of species and one part of the intestinal microbiota, along with other types, may be the cause of insulin resistance.
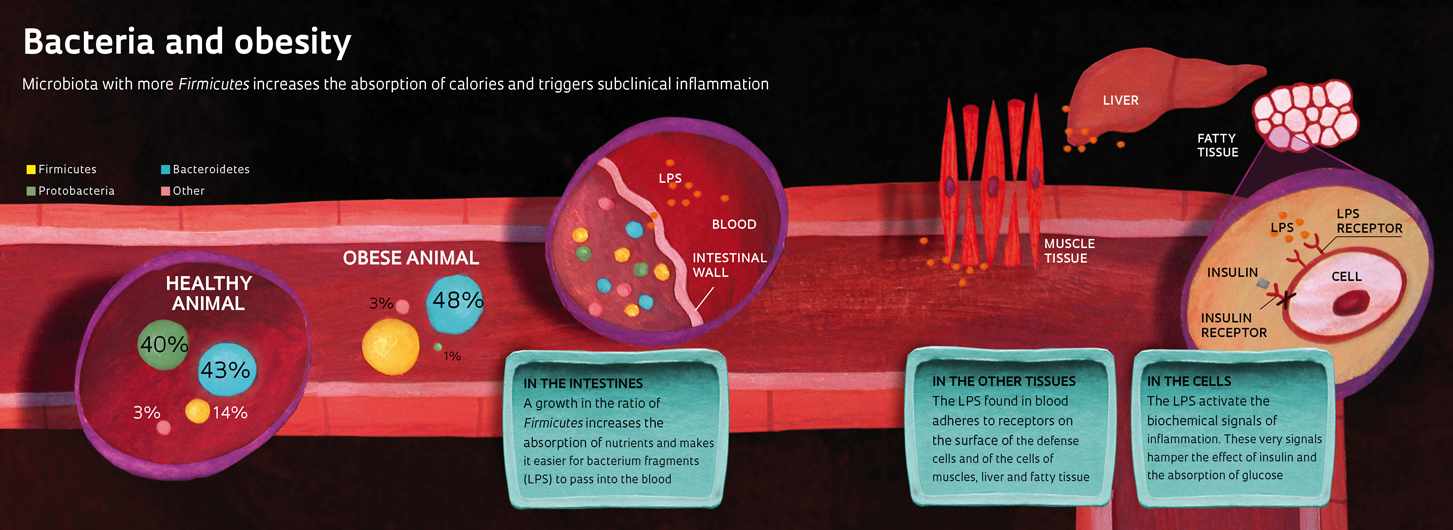
The proportional increase of Firmicutes in the microbiota seems to influence the development of diabetes and obesity in two ways. First, it improves the capacity to extract energy from food. Some Firmicutes species break long sugar molecules, called polysaccharides, found in cereal, fruit and vegetables, which otherwise would pass through the body unused. Secondly, the bacteria contribute to the development of a subtle inflammation, typical of obesity, which spreads through the body and interferes with insulin use.
“The intestinal microbiota isn’t the sole cause of diabetes and obesity; it’s probably not the most important one either,” commented Saad. “However, we found that it provokes an inflammation in the adipose tissue initiating an abnormal and persistent weight gain,” explains the researcher, whose team many years ago identified that this inflammation interferes with the brain functions controlling hunger and gratification (see Pesquisa FAPESP issue 140).
It is not the Firmicutes that spread the inflammation. For reasons that are unknown so far, these bacteria seem to facilitate the passage of small fragments of other bacteria through the delicate intestinal wall. These fragments, formed by sugar and fat molecules and known as lipopolysaccharides (LPS), pass through intestinal mucosa reaching surface receptors of different types of body cells.
Once connected to the macrophage membrane, i.e., the first defense cells that recognize invasive microorganisms and compounds foreign to the body, the LPS activate biochemical signals that place the immune system in a state of alarm, beginning a light inflammation tens of times weaker than that caused by bacteria entering the blood stream (aka, infection). An inflammation related to an infection can heal within days, but one caused by the LPS can last for years and affect the entire organism. LPS triggered inflammation signals in muscle cells, the liver and the adipose tissue also cause another distinct effect: they prevent the use of insulin and glucose uptake in the cells – insulin resistance.
Extended LPS exposure leads to insulin resistance, first in the liver and later in the muscles – the tissue that consumes the greatest amount of energy in the body. It is only later that the condition reaches the adipose tissue. This is why the body accumulates fat. Glucose that passes unused by the liver or the muscles lingers in the blood and is absorbed by the adipose tissue. “The cells in this tissue receive and store glucose as fat for a long time before they become insulin resistant,” explains Fábio Bessa Lima from the Adipose Tissue Physiology Laboratory at the University of São Paulo (USP).
It took four years of work to conclude that the Firmicutes could cause insulin resistance. Biologist Andrea Moro Caricilli from Saad’s laboratory had to carry out several tests on mice to identify the connection between the intestinal microbiota, inflammation and insulin resistance.
It all began in 2008, when Saad’s team got an unexpected result in an experiment with the rodents at Federal University in Minas Gerais by immunologist Ricardo Gazzinelli. The animals were genetically modified not to express a protein, which identifies foreign substances and sets off an inflammation known as toll-like receptor 2 or TLR2, on their membrane cells. At the time, Canadian and Swiss researchers showed that, even on a diet with a fat content ten times higher, the rodents without TRL2 became neither diabetic nor obese. Saad’s team, however, was unable to repeat the results. “When Andrea would show me the data, I’d say it was wrong. The animals, which theoretically should have remained slender, gained more weight than the norm,” said Saad.
The difference was partly explained by the conditions in which the animals were raised. The Swiss-Canadian mice without TRL2 lived in bacteria-free rooms and were fed sterile water and rations. Once out of this environment, they acquired intestinal microbiota and gained weight. The animals in Saad’s laboratory did not live in a sterile environment nor did they receive a high-calorie diet. Even though they received normal rations, they were already 50% heavier than the mice without the genetic modification at four months of age. They would have developed even more severe cases of diabetes and obesity if served a high-calorie diet.
After repeating the tests and finding that the animals had not been swapped, Saad and Andrea began to look for other possible explanations. As these animals had higher LPS levels in their blood and increased signs of inflammation, the researchers decided to analyze the rodents’ intestinal microbiota. The mice without TLR2 had developed a very distinctive microbiota that consisted of 48% of Firmicutes and 48% of Bacteroidetes. In comparison, the other animals’ microbiota comprised 14% of Firmicutes, 43% of Bacteroidetes and 39% of Proteobacteria.
This served as a good indication that the rest of the explanation could be found in the microbiota. In 2006, North American physician Jefferey Gordon’s team at the University of Washington observed that obese people’s microbiota differed from that found in healthy people. The microbiota in the obese was basically made up of Firmicutes and Bacteroidetes and with a much higher ratio of the former than that found in individuals with the recommended weight.
These findings set off studies about infectobesity, a line of research that emerged in 1988 and that tries to explain obesity unrelated to genetic changes, sedentary lifestyle and eating disorders in infections caused by pathogens (viruses, bacteria and other microorganisms). Despite recent advances, such as the mapping of the intestinal microbiota that identified nearly 400 species, there was still no good explanation as to why an obese person’s microbiota would be different from that of a slender one. “We don’t know if the microbiota profile changes as a result or as a consequence of obesity,” said Doctor Sandra Vivolo, a specialist in diabetes epidemiology at the USP School of Public Health.
The Unicamp team’s data suggested that mice without TLR2 developed insulin resistance and became obese after adapting a differing intestinal microbiota. As this needed to be confirmed, Saad and Andrea decided to run additional tests. Firstly, they used antibiotics to eliminate the animals’ intestinal microbiota. If this was in fact the cause of insulin resistance, killing the bacteria would diminish or eliminate the problem. At the end of a two-week antibiotics treatment, the amount of bacteria had reduced drastically and the ratio was similar to that found in animals without the genetic modification. Most importantly, the insulin sensitivity normalized and the rodent lost weight.
The connection between the microbiota, the development of insulin resistance and weight gain was shown. However, it was still unclear if the intestinal bacteria initiated the metabolism changes that were the cause of the problem. To put this idea to the test, Andrea transplanted the microbiota into rodents that did not produce TLR2 and that of slim animals into mice with simpler microbiota. Those who received the microbiota from rodents without TLR2, with high Firmicutes levels, became obese and diabetic. Those transplanted with microbiota from the test group did not change. “These results show that an environmental factor, such as microbiota, had dominance over the genetic protection” said Saad. “The microbiota is more important than we used to think.”
The PLoS Biology’s article points to new paths for diabetes and obesity cure and prevention. “We’re not suggesting the use of antibiotics to treat obesity; in our study, they served to prove an idea” warned Saad. Moreover, if used in obesity treatments, the antibiotics could possibly do even more harm than good. The microbiota’ functions are essential for the organism as the bacteria produce vitamins and enzymes that help metabolize fats. Furthermore, eliminating an unfavorable microbiota may make space for an even less favorable one.
Centers in Europe and the US transplant microbiota into human beings but only on an experimental basis and to treat serious infections. “Some encourage the use of these methods in other circumstances, but there is no data to support it yet,” said gastroenterologist Eamonn Quigley from University College Cork, in Ireland.
Even if the procedure were approved for obesity, there are no guarantees that it would work. “In the long term, the intestine has a tendency to be re-colonized by the original microbiota,” said Quigley. Some believe that probiotics, containing live microorganisms, may help develop weight-gain evading microbiota but this is yet to be proven. “Maybe it could work as a preventive measure before weight gain,” comments Saad.
In the meantime, as the tests continue, the safest bet is a diet low in fat, especially in red meat, and exercise. In 2010, Chinese researchers showed that fat consumption changes the microbiota make-up and leads to obesity. In December, a study in the British Journal of Nutrition found that consumption of fruit, vegetables, whole grains and fish reduces obesity’s characteristic inflammation.
The Project
National Obesity and Diabetes Institute (nº 08/57952-5); Modality Thematic Project; Coordinator Mário José Abdalla Saad – FCM/Unicamp; Investment R$ 3,292,062.55 (FAPESP)
Scientific article
CARICILLI, A.M. et al. Gut microbiota is a key modulator of insulin resistance in TLR 2 knockout mice. PLoS Biology. 6 Dec. 2011.