 EDUARDO CESARIt was 10:20 on the morning of Sunday, May 17 when Pedro, a thin and rather shy adolescent, slid into a magnetic resonance imaging machine at the Institute of Radiology at the University of São Paulo (USP). He had just finished answering a lengthy series of questions about his emotions and behavior at home, in school and with friends, and he would spend the next 40 minutes on his back in the machine, which would take almost 6,000 images of his brain. Pedro,17, is a member of a group of 2,512 children and adolescents from São Paulo and Porto Alegre–almost 60% of whom are at high risk for developing psychiatric disorders–who have been followed since 2009 by researchers at the National Institute of Developmental Psychiatry for Children and Adolescents (INPD). These young people are participating in a pioneering study in Latin America seeking to identify changes in the structure and function of the brain that characterize healthy maturation and those that indicate a risk for developing psychiatric disorders.
EDUARDO CESARIt was 10:20 on the morning of Sunday, May 17 when Pedro, a thin and rather shy adolescent, slid into a magnetic resonance imaging machine at the Institute of Radiology at the University of São Paulo (USP). He had just finished answering a lengthy series of questions about his emotions and behavior at home, in school and with friends, and he would spend the next 40 minutes on his back in the machine, which would take almost 6,000 images of his brain. Pedro,17, is a member of a group of 2,512 children and adolescents from São Paulo and Porto Alegre–almost 60% of whom are at high risk for developing psychiatric disorders–who have been followed since 2009 by researchers at the National Institute of Developmental Psychiatry for Children and Adolescents (INPD). These young people are participating in a pioneering study in Latin America seeking to identify changes in the structure and function of the brain that characterize healthy maturation and those that indicate a risk for developing psychiatric disorders.
The most significant findings of this research began to surface in recent months. The psychological, biochemical and neuroimaging data collected between 2009 and 2010 during the project’s first phase suggest that during the transition from childhood to adolescence, the brain systems of healthy young people undergo changes that look different from those taking place in children with a higher propensity for developing psychiatric problems. Doctors and other mental health professionals hope that once they have a detailed view of the changes that point to an undesirable evolution, they can use these indicators to determine the risk of mental disorders—signs that surface before a problem even becomes evident. If effective markers are discovered, it might be possible to intervene early to protect the brain and prevent an illness from arising.
“One day, we want to be able identify individuals with an elevated risk of mental disorders early on,” says Euripedes Constantino Miguel, a professor in the Department of Psychiatry at USP and the coordinator of the research study. “If we have the parameters to do so, we might be in a position to take actions that bring the brain back to a normal developmental trajectory.”

EDUARDO CESARExam of image done at USPEDUARDO CESAR
“This would completely transform the mental health field,” declares psychiatrist Rodrigo Bressan, coordinator of the Interdisciplinary Laboratory for Neuroimaging and Cognition (LiNC) at the Federal University of São Paulo (Unifesp), and the research coordinator at INPD responsible for project imaging and biomarkers, a facet in which researchers from the Federal University of Rio Grande do Sul (UFRGS) and the Federal University of the ABC (UFABC) are participating. “We still cannot predict the occurrence of mental disorders today. In most cases, psychiatrists are called in once the illness has taken hold, and treatment consists of prescribing medication and using psychotherapy to manage the symptoms and limit the damage they cause to the patient.”
Underlying the search for risk markers is the growing realization that mental disorders have a medical basis. “Psychiatric illnesses are no longer understood only as disorders of the mind or disturbances in behavior,” Bressan explains. “They are also diseases of the brain, a complex organ with enormous plasticity, which is highly influenced by the environment and by social interaction in particular.”
The most accepted theory in medicine and psychology explains mental disorders as a result of the interaction between the social, economic, psychological and cultural conditions in which an individual lives—the so-called environmental factors—and his or her propensity to develop a problem, driven by genetic factors. Progress in imaging studies has made it possible to see the brain in vivo and associate subtle changes in its structures—slightly higher or lower volume or an abnormal level of activation in a neuronal network—with changes in behavior. These changes are much more minute that those seen in neurodegenerative diseases like Parkinson’s or Alzheimer’s.

EDUARDO CESARStudy participant goes through a simulation before being subjected to magnetic resonance imagingEDUARDO CESAR
In a 2013 TED conference held in California, Thomas Insel, director of the National Institute of Mental Health in the United States, used the metaphor of urban transportation infrastructure to explain what happens in the brain in the case of mental disorders versus the case of diseases like Parkinson’s or Alzheimer’s. Neurodegenerative diseases lead to cell loss and major lesions, which would correspond to flooding in a city neighborhood or even the collapse of a viaduct. Mental disorders could be compared to a malfunction in the traffic signal network. Both problems disrupt traffic, but the former tends to lead to permanent damage while the latter can be readjusted more easily if it is detected early.
At the same time, epidemiological studies began to find evidence that mental health problems, in addition to being chronic, costly and very incapacitating, also begin early. In 2005, sociologist Ronald Kessler, a specialist in mental health epidemiology at Harvard University, published a study that shows that 50% of cases begin before the age of 14 and 75% before the age of 24. Taken together, this evidence supports the idea that psychiatric disorders result from neurodevelopmental problems. Recurrent physical and psychological abuse and other stressful events experienced in childhood and adolescence continually interact with genes that determine a child’s vulnerability to psychiatric problems, generating changes in the function and structure of brain networks. “Beginning at a certain point, the accumulated changes would be sufficient to produce the symptoms of psychiatric illness,” explains Miguel.
In the study involving children and adolescents from São Paulo and Porto Alegre, the researchers are comparing what is considered a healthy brain’s development trajectory (participants have no psychiatric symptoms) with individuals considered off track (those who have some sign of a mental disorder or children of individuals with a diagnosed psychiatric illness). By comparing these trajectories, they hope to find specific stages of maturation that will indicate who might get sick in the future. At the same time, they are trying to identify changes in the levels of compounds found in the blood and changes in emotions and behavior that might also be associated with the emergence of psychiatric disorders. In the long run, they hope to obtain a set of reliable risk markers for mental health, somewhat akin to what blood pressure and blood cholesterol levels represent for heart disease.
 “Heart disease does not begin with a blocked artery or heart attack but rather much earlier,” Bressan points out. “The same thing happens with psychiatric illness.” This is why psychiatrists and neuroscientists are trying to discover something that plays the same role for mental disorders as high cholesterol does for heart disease. The neural networks related to psychiatric symptoms organize and reorganize themselves more intensely during childhood and adolescence, after which they are consolidated, which makes it much more difficult to change them, even with medication and therapy. “The goal of identifying symptoms earlier, even before an illness begins to manifest itself, is to enhance the effectiveness of treatment, which is limited,” says psychiatrist Luis Augusto Rohde, professor at UFRGS and the project’s assistant coordinator. “Right now, medication works in only 60% of cases,” he says.
“Heart disease does not begin with a blocked artery or heart attack but rather much earlier,” Bressan points out. “The same thing happens with psychiatric illness.” This is why psychiatrists and neuroscientists are trying to discover something that plays the same role for mental disorders as high cholesterol does for heart disease. The neural networks related to psychiatric symptoms organize and reorganize themselves more intensely during childhood and adolescence, after which they are consolidated, which makes it much more difficult to change them, even with medication and therapy. “The goal of identifying symptoms earlier, even before an illness begins to manifest itself, is to enhance the effectiveness of treatment, which is limited,” says psychiatrist Luis Augusto Rohde, professor at UFRGS and the project’s assistant coordinator. “Right now, medication works in only 60% of cases,” he says.
Some mental disorders already have risk factors mapped out. Studies conducted abroad that followed subjects from childhood to adulthood have shown, for example, that physical and psychological abuse endured in early life and drug use in adolescence are associated with psychiatric problems later in life. By determining at what point brain development begins to deviate from the normal path, it may be possible to try to intervene—changing habits and other environmental factors—so that brain development returns to its normal trajectory. “We still know very little about how brain structures develop,” says Bressan.
 “We are starting to understand what shapes brain development because of large cohort studies [which follow the health of a population over a long period of time],” says neuroscientist Tomáš Paus, at the University of Toronto in Canada, who launched one of the world’s first mental health cohort studies 15 years ago. “This and other large longitudinal cohort studies provide a unique opportunity to examine the brain’s organization and development,” says Julia Zehr, of the Developmental Trajectories of Mental Disorders Branch at the National Institute of Mental Health in the US. “We still don’t know very much about brain development, particularly about developing neural circuits and the regions that influence them in a way that shapes their function,” says Zehr.
“We are starting to understand what shapes brain development because of large cohort studies [which follow the health of a population over a long period of time],” says neuroscientist Tomáš Paus, at the University of Toronto in Canada, who launched one of the world’s first mental health cohort studies 15 years ago. “This and other large longitudinal cohort studies provide a unique opportunity to examine the brain’s organization and development,” says Julia Zehr, of the Developmental Trajectories of Mental Disorders Branch at the National Institute of Mental Health in the US. “We still don’t know very much about brain development, particularly about developing neural circuits and the regions that influence them in a way that shapes their function,” says Zehr.
In the first phase of the Brazilian project, the researchers subjected 770 of the 2,512 participants to magnetic resonance imaging that evaluated the brain’s physical structures and mapped out the functioning of some brain networks. With the data in hand, statistician and neuroscientist João Ricardo Sato, of the Center of Mathematics, Computation and Cognition at UFABC, began to map how a healthy brain undergoes change during childhood and adolescence, focusing on the evolution of two brain networks: default mode and cognitive control.
Opposing and complementary
More active when someone is at rest, and can allow the mind to wander, the default mode network is associated with a person’s ability to withdraw into an inner world of self-reflection (introspection) and recall important life events (autobiographical memory), such as where one’s first kiss took place. The cognitive control network, on the other hand, comprises areas of the brain that are activated when attention must be focused on the external world—for example, taking a test, doing a calculation, or suppressing inappropriate behavior like throwing a spit ball at a professor’s back.
 These two networks function in opposition to each other: when one is more active, the other quiets down, and vice-versa. Sato used tools from an area of mathematics called graph theory to evaluate how the features of these two networks change as a person ages. This approach treats the brain’s regions as if they were points or nodes in a network and the simultaneous activation (functional connectivity) of the two regions as if it were a path connecting two points. This strategy has an advantage compared to data analysis methods normally used in health-related studies: it allows for a comprehensive view of the organization of the brain’s connectivity networks.
These two networks function in opposition to each other: when one is more active, the other quiets down, and vice-versa. Sato used tools from an area of mathematics called graph theory to evaluate how the features of these two networks change as a person ages. This approach treats the brain’s regions as if they were points or nodes in a network and the simultaneous activation (functional connectivity) of the two regions as if it were a path connecting two points. This strategy has an advantage compared to data analysis methods normally used in health-related studies: it allows for a comprehensive view of the organization of the brain’s connectivity networks.
Analysis of the brain images of 447 children between the ages of 7 and 15 with no sign of psychiatric disorders revealed that, in general, the connection between the points on these networks become stronger with age. This means that communication between these areas of the brain becomes stronger and synchronized. “Previous studies that evaluated variations in the volume of brain structures already indicated that this should happen,” says Bressan. “Now we have captured these changes taking place in a functioning brain,” he says.
The internal hierarchy of these networks also changes between late childhood and early adolescence. Some areas become more important while others become less so. Sato noted, for example, that the medial prefrontal cortex—the area of the brain associated with abstract thought, planning and control—played a bigger role in older study participants. This also occurs with two areas of the cingulate gyrus, a deeper fold in the cerebral cortex linked to the regulation of emotions and attention, the capacity to create social connections and to anticipate and avoid unpleasant situations. With age, the anterior and posterior regions of the cingulate begin to mediate the connection between many areas of the two networks, acting as a junction between very busy highways.

Andreas Horn / Max Planck Institute for Human Development / Wikipedia
Highly integrated network: brain regions that form the default mode network (yellow) and the fibers that connect themAndreas Horn / Max Planck Institute for Human Development / WikipediaChanges in the level of activity in these networks reflect what is known about human emotional and cognitive development. From childhood to adolescence, subtle anatomical characteristics of some areas change, as does the way in which they communicate with each other. These changes are accompanied by the development of new skills. In early childhood, a child develops motor capacity, and when he reaches the age of 5 or 6, he is ready to learn to read and write. By the age of 9, he has now refined his ability to communicate verbally and begins to develop the capacity to think in more abstract mathematical terms. From then until he reaches adulthood, he gains increasing control over his impulses and emotions. “Children are much more impulsive than adolescents, since subcortical areas of the brain [which are deeper and evolutionarily more primitive] are primarily activated,” explains biologist Andrea Jackowski, specialist in neuroimaging at LiNC and one of the study’s main contributors.
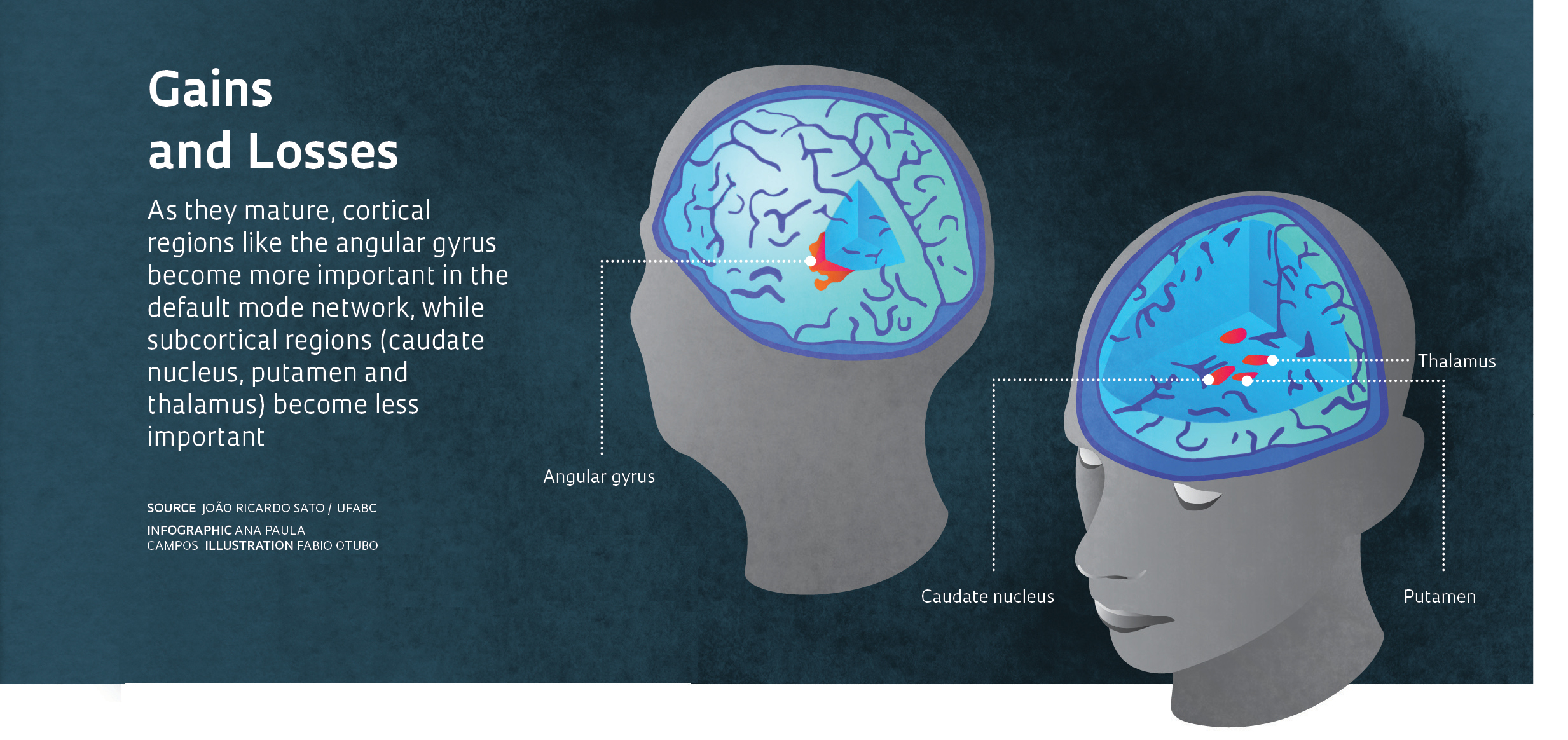
To gain an overview of the changes in the brain, Sato simultaneously compared the development of activity patterns in 325 regions that have already been mapped out by specialists in brain anatomy. Put simply, what is different between a child and an adolescent is that the angular gyrus—a region in the brain’s cortex involved in important tasks like language and mathematical processing, keeping focused, and memory recall—plays a greater role in adolescents. At the same time, some structures in a region that is deeper within the brain and in evolutionary terms more primitive—the basal nuclei, which integrate emotional and motor information—become less important.
One finding enthralled researchers owing to its potential clinical application. After determining how the default mode network matures in healthy subjects, Sato and his fellow researchers decided to analyze changes in this network in the brains of children and adolescents with symptoms of psychiatric problems. Previous studies had already associated changes in the network’s functioning with depression and anxiety, which were marked by symptoms connected to introspection, like the tendency to obsess excessively about problems.
If changes in this network’s functioning were associated with changes in behavior and psychiatric disorders, wouldn’t the symptoms that manifested in some children signal problems in the network’s maturation process? To answer this question, researchers needed to determine how the network evolved with age and which changes were unexpected. This is a complicated task, since variations in brain activity are significant in healthy people and can be unpredictable in people with psychiatric disorders.
Sato, who earned an undergraduate degree in statistics and worked in finance before he became interested in neuroscience during his PhD studies, decided to attack the problem using a computational model, machine learning, which was adopted to develop tools that can automatically learn and recognize patterns after being exposed to just a few examples, like filters for unwanted e-mail messages.
He created a computer program to recognize the pattern of spontaneous activity in the default mode network in children of different ages. He then used it to evaluate delays in the maturation process of the brain network in 622 children and adolescents who had undergone functional magnetic resonance imaging. The combination of the tools available from graph theory and machine learning led him to create a brain maturity index, described in an article accepted by the Journal of Child Psychology and Psychiatry. This index takes into consideration the fact that, as already observed by the Brazilian group, and in smaller samples by foreign researchers, brain networks change with age. By comparing the maturity index obtained by the program with information on symptoms identified through questionnaires answered by parents of the study’s participants, Sato verified that children and adolescents with more signs of psychiatric problems had more immature brain networks.
How immature? Sato has not yet completed his calculations, but he estimates that the delay in maturity is between two and three years. This can mean that the default mode network of a 10-year-old child who has serious psychiatric symptoms could have the same level of maturity of a healthy 7- or 8-year-old child. Children and adolescents with a less mature default mode network generally had symptoms classified as internalizing, often depression and anxiety. “The conventional tests used to analyze data from magnetic resonance images would not have allowed us to extract this kind of information,” says Euripedes Miguel. “This was only possible by putting together these more advanced statistical strategies.”
This finding is important not just because it makes it possible to measure the maturation of this network, whose function is not yet well understood. It is also relevant because of its potential use in psychiatric treatment. If the index should demonstrate its effectiveness in the next stages of this project and in other studies, it could be used as a way to assess the risk for future psychiatric problems. “A risk marker of this type would mean that imaging would serve a new purpose in psychiatry,” says physician Giovanni Salum at UFRGS, who coordinated the data collection process in Porto Alegre. “Today, imaging is used only to rule out potential problems like tumors or lesions.”
“This indicator points toward the eventual development of a risk marker, but to earn this distinction, it would have to have a very high predictive value,” Sato believes.
Miguel thinks that the solution will not be just one marker. “We will probably need a set of markers: imaging, biochemical and behavioral,” he says. This is why researchers are looking for a connection between clinical indicators of psychiatric illness and changes in the level of compounds in the blood, in addition to the association between brain imaging and symptom data.
At Unifesp, psychiatrist Elisa Brietzke and her team analyzed blood samples collected in recent years from 600 children who participated in the neuroimaging study conducted in the first phase of the study. They were looking for compounds that might indicate changes in the brain associated with a higher risk of developing psychiatric illnesses, and which might act as biochemical risk markers. So far, they have identified two candidates: eotaxin, a chemical communicator associated with inflammation; and tumor necrosis factor receptor 2, known as TNFR2, a molecule that appears to prevent brain cell death.
The data presented at the annual meeting of the Society of Biological Psychiatry, held in May 2015 in Canada, show that at the same time as levels of eotaxin were higher in the blood of children and adolescents with more symptoms of psychiatric problems, levels of TNFR2 were lower. According to Brietzke, this combination was able to identify with a reasonable degree of precision children of women who while pregnant had consumed alcohol, which has a powerful effect on the fetal nervous system. Children and adolescents of parents with mood disorders (depression or bipolar disorder) had more elevated levels of eotaxin in the blood, while those with parents who had anxiety disorders (phobias, panic disorder or anxiety) showed lower levels of the neuroprotector TNFR2.
Alongside the work of Sato and Brietzke, clinical researchers are investigating ways to use the information collected from mental health surveys to identify behaviors that serve as early indicators of a deviation in the trajectory of brain development. One example is the work of psychiatrist Pedro Pan, a researcher at LiNC, who is studying bipolar disorder, which is characterized by alternating episodes of depression and mania and which is difficult to diagnose in children and adolescents. He divided the 26 symptoms that appeared in 479 children and adolescents with signs of mania in two large groups: exuberant subjects, which includes, for example, individuals who are excessively animated, speak quickly and are full of energy; and those who have a low threshold of self-control, a group that includes people with such things as signs of excessive irritation, difficulty controlling their thoughts and little regard for danger. In comparing the two classifications of symptoms with the harm they caused in the children’s lives (according to accounts by their parents), they verified that symptoms associated with low self-control allowed them led to identify more serious cases that probably required treatment.
Researchers hope to bolster their initial findings when they analyze data from the project’s second phase, which were collected since late 2013. By mid-May, the São Paulo and Porto Alegre teams, which include almost 30 researchers combined, had already completed the neuropsychological evaluation conducted at home of almost 2,000 participants, almost 80% of the total number surveyed in the project’s first phase. Of the 770 boys and girls who had undergone the magnetic resonance imaging exams in 2009 and 2010, almost 300—including Pedro—had already had the exam for a second time by May. Another 300 will be imaged before the end of the year. “When we compare data from the first phase to the data we are currently collecting,” says João Sato, “we will get a more accurate perspective.” By comparing the data, researchers should be able to confirm whether the people at-risk do indeed develop psychiatric problems.
Projects
1. National Institute for Developmental Psychology: a new approach for psychiatry focusing on our children and their futures (No. 2008/57896-8); Grant Mechanism Thematic Project – INCT; Principal Investigator: Euripedes Constantino Miguel Filho (IPq-FM-USP); Investment: R$5,695,960.92 (FAPESP and CNPq).
2. High risk cohort study for psychiatric disorders in childhood: 3-year follow-up neuroimaging study (No. 2013/08531-5); Grant Mechanism Regular Research Grant; Principal Investigator: Andrea Parolin Jackowski (Unifesp); Investment: R$316,708.90 (FAPESP).
3. Machine learning in neuroimaging development of methods and clinical applications in psychiatric disorders (No. 2013/10498-6); Grant Mechanism Regular Research Grant; Principal Investigator João Ricardo Sato (UFABC); Investment: R$110,925.07 (FAPESP).
Scientific articles
SALUM, G. A. et al. High risk cohort study for psychiatric disorders in childhood: rationale, design, methods and preliminary results. International Journal of Methods in Psychiatric Research. Dec. 2014.
SATO, J. R., et al. Age effects on the default mode and control networks in typically developing children. Journal of Psychiatric Research. Nov. 2014.
SATO, J. R., et al. Decreased centrality of subcortical regions during the transition to adolescence: a functional connectivity study. Neuroimage. Jan. 2015.
SATO, J. R., et al. Default mode network maturation and psychopathology in children and adolescents. Journal of Child Psychology and Psychiatry. May 2015.
PAN, P. M., et al. Manic symptoms in youth: dimensions, latent classes, and associations with parental psychopathology. Journal of the American Academy of Child and Adolescent Psychiatry. 22 Mar. 2014.