Immunizations begin in Brazil with CoronaVac, the first available vaccine; experts explain the controversies around its data
Nurse Mônica Calazans was the first person to receive CoronaVac outside of clinical trials, initiating vaccinations in Brazil against Covid-19
Rodrigo Paiva / Getty Images
Exactly 180 days after the Chinese pharmaceutical company Sinovac and the Butantan Institute of São Paulo initiated the phase 3 trial for Profiscov, the vaccine was given to a common Brazilian. The trial’s purpose was to evaluate the effectiveness and safety of the CoronaVac vaccine, made from inactivated virus, for about 13,000 Brazilian health care professionals. On January 17, the first person to receive it was nurse Mônica Calazans, 54, who works at the Intensive Care Unit (ICU) at the Emílio Ribas Infectology Institute in São Paulo.
This event marked the beginning of vaccinations in Brazil and was attended by São Paulo governor, João Doria. It took place minutes after the Brazilian Health Regulatory Agency (ANVISA) temporarily authorized the emergency use of CoronaVac and the vaccine Covishield, created by the Swiss-British laboratory AstraZeneca along with Oxford University in the United Kingdom, and produced by the Serum Institute in India. The regulatory agency agreed that the population could receive the six million doses imported from China by Butantan and two million doses of the Oxford vaccine, which the Brazilian government bought from India.
When ANVISA’s Board of Directors made their decision, they made the use of CoronaVac conditional on the Butantan Institute signing an agreement of engagement, which it must submit by the end of February, including data on the vaccine’s immunogenicity. Immunogenicity is the capacity of a disease-causing agent to induce a host to produce antibodies, primarily neutralizing antibodies, in addition to stimulating the immune system’s cell growth. “This data is fundamental to confirm the duration of the immunological response in vaccinated individuals,” informs ANVISA.
The endorsement for CoronaVac was given at the end of a week when the vaccine was at the center of a controversy about its efficacy. The São Paulo government announced on January 12 that the vaccine had a global efficacy of 50.38%, a rate slightly higher than the 50% threshold recommended by the World Health Organization (WHO) and key regulatory agencies around the world. Six days earlier, state authorities had made an initial announcement about vaccine effectiveness, highlighting that CoronaVac had reduced by 78% the risk of those with the disease requiring medical assistance and confirmed 100% protection against moderate and severe cases. However, in these cases, there was a need for a greater number of observations.
Experts have criticized and questioned the capacity of the vaccine to slow down the pandemic in Brazil due to the delay in communicating the numbers—in two phases—the lack of information in communicating initial rates, when it was not clear if the 78% and 100% rates referred to a study segment, and the fact that the global efficacy of CoronaVac, 50.38%, was lower than that of other Covid-19 vaccines.
Final phase of CoronaVac production at the Butantan InstituteButantan Institute
Scientific studies published previously have already demonstrated that the BNT162b2 vaccine—made by the North American pharmaceutical company Pfizer and the German biotechnology startup BioNTech—will reach an efficacy rate of 95%, while the laboratory-made vaccine by North American Moderna, named mRNA-1273, would reach 94.1%. Both results were communicated in December in the New England Journal of Medicine. The formulation by AstraZeneca/Oxford, which are also partnered with Brazil’s Oswaldo Cruz Foundation (FIOCRUZ) in Rio de Janeiro, will have an average efficacy of 70.4%, according to another article published in December in the journal The Lancet. Experts advise, however, that the efficacy of the vaccines is not directly comparable as the clinical studies used different methodologies, as we will explain below.
Selling feature Pesquisa FAPESP heard from immunologists, virologists, infectologists, and epidemiologists to clarify doubts around the efficacy of CoronaVac. First, the researchers unanimously confirmed that, given the situation with the disease in Brazil, it is an adequate vaccine that is both effective and safe. The Butantan Institute reported that there have been no serious side effects associated with this formulation.
“CoronaVac’s selling feature is the 78% reduction in the number of Covid-19 cases that require medical care and hospitalization,” says infectologist Raquel Stucchi from the School of Medical Sciences at the University of Campinas (FCM-UNICAMP). “With its global efficacy at 50%, if we have today an average of 60,000 cases per day in Brazil, this number should drop by half as the vaccine is distributed. At this moment in the pandemic, this is fantastic.”
Immunologist Ricardo Gazzinelli, president of the Brazilian Society of Immunology (SBI), has had a similar assessment. “Even though the number of events (individuals in the study who have manifested Covid-19 symptoms and who have tested positive for the virus) needs to be increased, the trend among those who have been vaccinated is a reduction in moderate and serious cases requiring hospitalization. Furthermore, the number of people who need non-hospitalized medical care has been significantly reduced among those who have taken the vaccine. “These are key results,” notes Gazzinelli, researcher at the Translational Medicine Unit of FIOCRUZ, located at the University of São Paulo’s Ribeirão Preto School of Medicine (FMRP-USP).
According to biologist Flávio da Fonseca, president of the Brazilian Society of Virology (SBV) and professor at the Biological Sciences Institute of the Federal University of Minas Gerais (ICB-UFMG), CoronaVac could reduce the mortality rate of SARS-CoV-2 in Brazil and the public health problems created by the pandemic. “This is the worst health crisis in the last 50 years and, until recently, there was no solution for the Brazilian context. With a vaccine that reduces the chances of someone falling ill by 50% is better than not having a vaccine at all,” he says.
Researchers highlight that certain vaccines of the National Immunization Program (PNI) have similar efficacy to that of CoronaVac. “This is the case with the flu vaccine, which Brazilians take every year. Its efficacy is about 40% to 60%,” notes Fonseca. Other examples are the vaccines for rotavirus—which attacks the digestive tract and causes serious dehydration—with an approximate efficacy of 50%, and BCG—for the prevention of tuberculosis (TB)—with a rate between 60% and 80%.
“BCG impedes the emergence of the disease, as does CoronaVac. You may get infected, but the illness does not evolve, or will produce light symptoms,” clarifies Fonseca. “There are few vaccines that totally block the establishment and replication of the virus in an organism. The majority prevent the disease. The infection may take hold but without clinical relevance or appearance of symptoms.”
Studies of the first vaccines developed for the novel coronavirus have not assessed the capacity of the vaccines to block infection. “The current search for Covid-19 vaccines is focused on controlling symptoms. Over time, we will be able to focus on finding immunity that will protect us from infection. Not one of the present studies is measuring this, but concern for this will most certainly come after controlling the disease and reducing hospitalizations,” noted by SBI in a memo about the efficacy of the Covid-19 vaccines.
“It is odd that no study has measured the capacity of the vaccines to prevent infection,” remarks immunologist Cristina Bonorino, member of the SBI’s scientific committee and professor at the Porto Alegre Federal University of Health Sciences (UFCSPA) in Rio Grande do Sul. “At the beginning of the pandemic, when the pharmaceutical companies launched their studies, the scientific community asked that they also measure infection and not just the disease. The answer was that this was inviable as it would require testing all volunteers on a weekly basis using the gold standard molecular test for virus detection (PCR), leading to delays in concluding the studies.” The procedure would also increase the costs of testing.
Ideally, the vaccines should block infection as well as the disease. However, it is possible to reach herd immunity if many people are vaccinated against Covid-19, which would make it difficult for the virus to circulate. The majority of vaccines being used today only protect against the development of a disease, such as the measles vaccine and BCG for TB.
Shipping of batches of the vaccine to Brazilian statesRodrigo Paiva / Getty Images
Rate calculation Another point that generated questions and sparked attention on social media was a calculation used by the Butantan Institute to achieve the 50.38% efficacy rate for the vaccine. In an article titled “What is the true efficacy of CoronaVac?”, published in the newspaper O Estado de S. Paulo, biologist Fernando Reinach challenged the rate announced by the institute. “I decided to look at the data very carefully and, with the assistance of friends who are epidemiologists and engineers, I recalculated them. […] And the result was that the efficacy, as defined in any book about epidemiology, is 49.69%,” wrote Reinach.
For epidemiologist and infectologist Marcelo de Carvalho Ramos, of FCM-UNICAMP, the rate reported by Butantan—and later confirmed by ANVISA—is correct. In his opinion, the calculation that resulted in 49.69% was wrong to consider only the absolute number of participants and of illnesses in each of the study’s two groups, that which took the placebo (innocuous substance) and that which received the vaccine. According to Ramos, another variable should also be considered: the time that each volunteer was at risk of contracting Covid-19.
To understand the difference, to the decimal, it must be understood that the analysis of vaccine efficacy included 9,252 participants who were selected from the 12,508 volunteers who had received their second dose of the vaccine or of the placebo at least two weeks prior. Of the total, 4,653 received the two doses of the vaccine and 4,599 received the placebo. In the study, 252 Covid-19 cases were detected, with 85 infected in the vaccinated group and 167 in the control group.
With the method that only considers the absolute number of participants and diseases, the formula is simple. First, it is necessary to calculate the so-called disease incidence rate in each of the two groups. This is done by dividing the number of people who are ill by the total number of volunteers in each group. In the case of CoronaVac, the rate of incidence in the control group (CIC) was 3.6312%, while among those vaccinated (CIV), it was 1.8267%. The next step is to subtract the rate of incidence of those who are vaccinated (CIV) from the rate of disease incidence in the nonvaccinated individuals (CIC). The obtained result (1.8045%) should be divided by the rate of incidence in the nonvaccinated (3.6312%) group. After doing the calculations, you arrive at an efficacy rate of 49.69%.
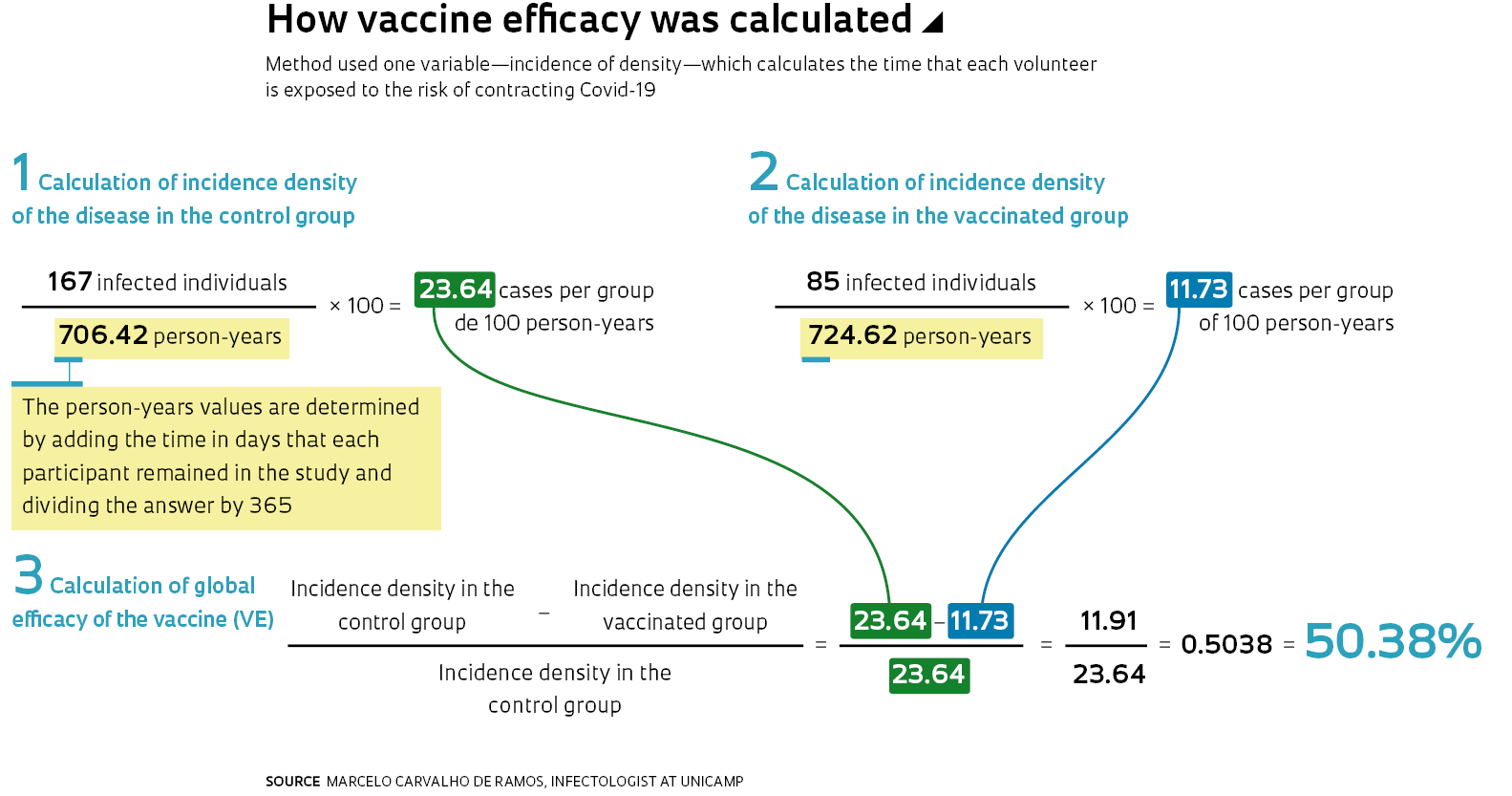
However, as Ramos explains, the fact that the length of time varies for the volunteers’ exposure to the risk of contracting the disease, since they enter the study at different points in time, we should use the person-years calculation rather than the absolute number of individuals exposed to the risk of infection. “This is done by adding the time in days that the participants in each group remain in the study and dividing the result by 365. If two patients remain in the study for six months, they constitute one patient-year. The resulting incidence rate is also called the incidence density,” explains the infectologist from UNICAMP.
Butantan reported that there were 724.62 person-years in the vaccinated group and 706.42 person-years in the control group. If you do the calculation using the aforementioned formula, substituting the number of participants of each group with the respective number of person-years, you will arrive at the 50.38% efficacy rate identified by the study (see infographic).
Upon submission of clinical trial protocols to regulatory agencies, pharmaceutical companies should report the method used to calculate efficacy of the product under development. Methodological selection should be defined and communicated before initiating testing to allow for an impartial assessment of the resulting data. In the CoronaVac study, being of short duration and where the time of virus exposure for volunteers can vary significantly, Butantan found the calculation based on incidence density to be more accurate.
Others in the spotlight Butantan was not alone in providing explanations about the efficacy of its vaccine. Upon reporting the preliminary study results of their vaccines, AstraZeneca and the University of Oxford were severely criticized. An error in the study caused some of the volunteers to receive a half dose of the vaccine followed by a complete dose when the expectation was to receive two doses.
As a result of the error, three efficacy rates were presented: 62%, for those who received two complete doses; 90%, for the group initially vaccinated with a half dose; and 70%, an average of the two previous indices. The calculation was contested by part of the scientific community. Furthermore, it was considered surprising that the efficacy resulted from a combined assessment of studies with distinct protocols from various countries (United Kingdom, Brazil, and South Africa). “The calculation yielding 70% as an average of the two different regimes is not correct as one of them was not part of the clinical study plan,” confirms Bonorino.
More recently, researcher Peter Doshi, of the University of Maryland School of Pharmacy in the United States, and associate editor of BMJ, the scientific journal of the British Medical Association, questioned the transparency of the data related to the Moderna and Pfizer vaccines. In an opinion article published in BMJ, he identified what he considered to be inconsistencies in the studies, primarily that of vaccine BNT162b2.
Vaccination of an indigenous woman in a village in MaricáBuda Mendes / Getty Images
According to Doshi, Pfizer did not include in the efficacy calculation thousands of cases in the clinical trial that were classified as “suspected Covid-19”—people with symptoms of the illness, but that had not been tested to prove virus infection. A document of the Food and Drug Administration (FDA), the regulating body for medications and foods in the United States, identified “3,410 suspected cases, but not confirmed for Covid-19, in the study’s total population, 1,594 occurring in the vaccinated group, and 1,816 in the placebo group.” “Based only on symptoms, it seems plausible to me that the efficacy of the Pfizer vaccine is below the 50% limit,” says Doshi to Pesquisa FAPESP.
The editor of BMJ identified other problems, based on an analysis of the FDA document, such as the exclusion of 317 individuals from the Pfizer study for reasons of “variance from protocols,” without the pharmaceutical company having to provide more details. Doshi asked the laboratory for answers but has not yet received a response. “They did not release their data. In the best-case scenario, they intend to share it in a year and a half, when the studies are completed.”
Another controversy around CoronaVac came out of the comparison of its Covid-19 efficacy with that of others. After all, why would you take a vaccine with 50% efficacy when there are others with more than 90%? Researchers understand that people have this question, but they maintain that it is not possible to directly compare the efficacy of the vaccines since the methodology used by the pharmaceutical companies in the clinical trials is not the same.
The Butantan, Pfizer, Moderna, and AstraZeneca/Oxford studies overlap on one point: they share the objective of evaluating the protection offered by their vaccines against Covid-19. “The primary outcome of the trials was the clinical manifestation of the disease in the volunteers,” explains Gazzinelli of the SBI. What happened is that the detail of the primary outcome—the definition of the symptoms that should be considered for subsequent PCR molecular testing to confirm infection by SARS-CoV-2—differed among the trials.
In the case of CoronaVac, it was established that the volunteers with the disease would manifest one of 11 symptoms, including migraine, runny nose, diarrhea, headache, shortness of breath, and cough. This would be followed by a diagnostic test using PCR to confirm infection. In other studies, a PCR was also necessary to confirm infection, but fewer symptoms were considered to define the disease (see infographic).
“Sinovac and the Butantan Institute used a very sensitive criterion for disease diagnosis. If the volunteer had a single symptom, even if negligible, such as fatigue or runny nose, they would do the PCR. The other vaccines were less rigid,” says Stucchi. “Furthermore, the volunteers were health professionals, a group with higher risk of contracting SARS-CoV-2.” For the UNICAMP infectologist, when CoronaVac is applied en masse, its efficacy can be even greater than that revealed by the study because the general population is less exposed to the virus. “Perhaps we will be finally able to turn Covid-19 into a little flu.”
This article may be republished online under the CC-BY-NC-ND Creative Commons license. The Pesquisa FAPESP Digital Content Republishing Policy, specified here, must be followed. In summary, the text must not be edited and the author(s) and source (Pesquisa FAPESP) must be credited. Using the HTML button will ensure that these standards are followed. If reproducing only the text, please consult the Digital Republishing Policy.