The daily routine of 19-year-old Giuliano Ferrer Piccolo would have been unthinkable for many youths with Down syndrome in the past. On Mondays, he takes drum lessons. Other weekdays are organized into a schedule that includes physical education, drama classes and a preparatory course for his first job, in addition to therapeutic follow-up sessions and some more drumming, for good measure. People with Down have a better quality of life today, but they still face difficulties when caring for their health. As children and adolescents, they must commonly deal with disorders related to excess weight, a result not only of clinical conditions typical of those with the syndrome, but also a lack of weight and height reference tables tailored for people with Down.
Giuliano started adding more movement to his routine and losing weight about four years ago, when he joined 937 fellow teenagers and children with Down, ranging in age from just a few weeks old to 20 years old, in a project conducted by the research group led by pediatrician Gil Guerra Júnior at the University of Campinas School of Medicine (FCM-Unicamp). Their goal was to measure the participants’ weight, height, head circumference and body mass index (BMI) and use the data to develop up-to-date growth charts specific to this population in Brazil.
Presented in two scientific papers published in 2017, these charts are fundamental tools for identifying deviations from what is considered healthy growth, and they allowed Giuliano’s mother and his doctor to verify that his weight was above average, even for a teenager with Down. “These follow-ups encouraged us to work on Giuliano’s diet at home and with his pediatrician, to have him lose weight until he reached the ideal level for boys his age who have the same syndrome and who experience a similar reality,” says his mother, Cleusa Ferrer.
The Down growth charts produced by the research group in Campinas are not the only ones, nor are they the first ever produced, but they are proposed as being more up-to-date and comprehensive for Brazilian children and adolescents with Down syndrome, the genetic disorder caused by having an extra copy of chromosome 21, affecting 3 to 14 out of every 10,000 children. When monitoring children with Down up to the age of 24 months, the Brazilian Ministry of Health currently recommends the use of growth charts developed by physician Zan Mustacchi during his doctoral studies at the University of São Paulo (USP) and presented in 2002. For ages 2 to 18, the Ministry advises using growth charts for children and teens with Down developed in the 1980s in the United States. “These charts may not be representative of the current growth patterns shown by children and adolescents with Down syndrome in a wider age range, such as the one covered in our study,” says physical educator Fabio Bertapelli. Bertapelli is a scientific advisor collaborating with the São Paulo State Federation of Associations of Parents and Friends of the Mentally Disabled (APAEs). With funding from the Brazilian Federal Agency for the Support and Evaluation of Graduate Education (Capes), he developed Brazil’s new growth charts for children and adolescents with Down during his doctoral studies, advised by Guerra Júnior at Unicamp and by Stamatis Agiovlasitis at Mississippi State University in the United States.
Children with Down often suffer from medical conditions that compromise their quality of life, including congenital heart diseases, hypothyroidism, gastrointestinal disorders and obstructive sleep apnea, in addition to stunted growth and excess body weight. On account of these health issues, according to the researchers at Unicamp, it is important for parents and doctors to rely on growth and development references that are closer to the reality of Brazilian children and teenagers with Down.
“Low stature in childhood and adolescence, low weight in the initial years of life and excess weight after age 2 are the most common characteristics shared by individuals with the syndrome,” explains Guerra Júnior. “These children and teenagers show growth patterns that are different from those published by studies performed in the past, both for populations with and without Down syndrome.”
Shorter
To draw the curves for the new charts, the researchers examined 10,516 weight, height and head circumference measurements taken from 938 children and adolescents with Down who attended the Outpatient Center for Integration of Pediatric Specialties at Unicamp, as well as 50 other care centers for people with Down syndrome in the state of São Paulo. Whenever possible, they added the previous measurements noted on the medical records or health booklets of each child.
When compared to people without the syndrome, the study participants were shorter at all ages. The average height gap increased in early adolescence and peaked at ages 17 to 19. Brazilians with Down within this age range are roughly 20 centimeters shorter than teenagers without the syndrome – in the United States, teens with Down, particularly males, are slightly taller than their Brazilian peers.
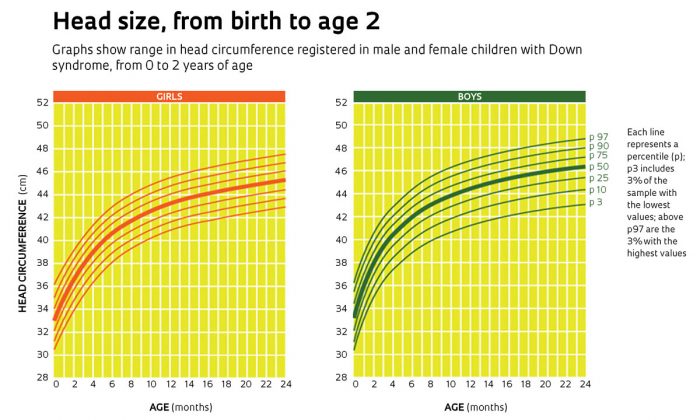
Children with Down also have smaller head circumferences in their first two years, and their body weight is lower until 15 months of age. But after that, they gain weight more rapidly and, from ages 3 to 18, their BMI values are higher than those of children and adolescents without the syndrome. “There are around 15 growth charts available for children and adolescents with Down,” says Bertapelli. “Almost every one of them advises that they tend to be overweight or obese, but none of them shows that these children gain less weight until their second year of life.”
The charts produced by the research group at Unicamp indicate that from birth to six months, Brazilian children with Down were up to 1.4 kg lighter than the averages for boys and girls without the syndrome. This is a worrisome finding because the first two years of life are a critical period in which many organs and tissues are still developing – the brain, for example, reaches 70% of its final volume in a child’s second year. Population studies on children without Down in the city of Pelotas, state of Rio Grande do Sul, suggest that rapid weight gain at this life stage is transformed into bones, muscles and organs, such as the liver and central nervous system. After this stage, rapid weight gain generates fatty tissue (See Pesquisa FAPESP Issues No. 179 and 208).