Based on its proven efficacy for epilepsy, cannabidiol has become the target of intensive research
After receiving judicial authorization, many families are using a domestic extract as treatment
Léo Ramos Chaves
Certain types of epilepsy do not respond to existing medications, subjecting children and adults alike to a succession of convulsive episodes that impede development and enjoying normal lives. For these cases, the use of cannabidiol (CBD), a substance produced by the Cannabis sativa plant, is becoming increasingly popular around the world. A growing number of potentially therapeutic uses for CBD and other compounds originating from marijuana, called cannabinoids, are not yet as well founded, but are receiving increased attention from researchers. Such is the case for various types of chronic pain, anxiety, post-traumatic stress, autism, Alzheimer’s, schizophrenia, and other illnesses for which pharmacies offer only limited help.
Results from international studies published in scientific articles corroborate the efficacy of cannabidiol as an adjuvant in epilepsy treatments, according to a systematic review published in 2018 in the Journal of Neurology, Neurosurgery & Psychiatry, by a research group led by Australian epidemiologist Louisa Degenhardt at the National Drug and Alcohol Research Centre in Sydney. In another review published in December 2019 in Lancet Psychiatry, she warns of a lack of convincing data to justify the widespread use of cannabinoids for depression, anxiety, psychosis, and other psychiatric disorders. The meta-analysis that her group conducted, however, included studies investigating the use of both the entire plant and of its isolated compounds, the majority of which studied THC as the active ingredient. Their conclusions emphasize the need for further studies.
Some of the studies cited in the reviews were done at USP, which figures prominently in works done using cannabidiol; Brazilian researchers do not have access to THC. According to the Web of Science platform, the São Paulo institution accounts for about 7% of global scientific production on the subject, followed by research centers in Israel, the United Kingdom, and the United States. Brazil’s ranking is primarily due to research by groups led by psychiatrists Antonio Zuardi, José Alexandre Crippa, and Jaime Hallak, and pharmacologist Francisco Silveira Guimarães, all at the Ribeirão Preto campus of the University of São Paulo (USP-RP) (see Pesquisa FAPESP issue no. 125).
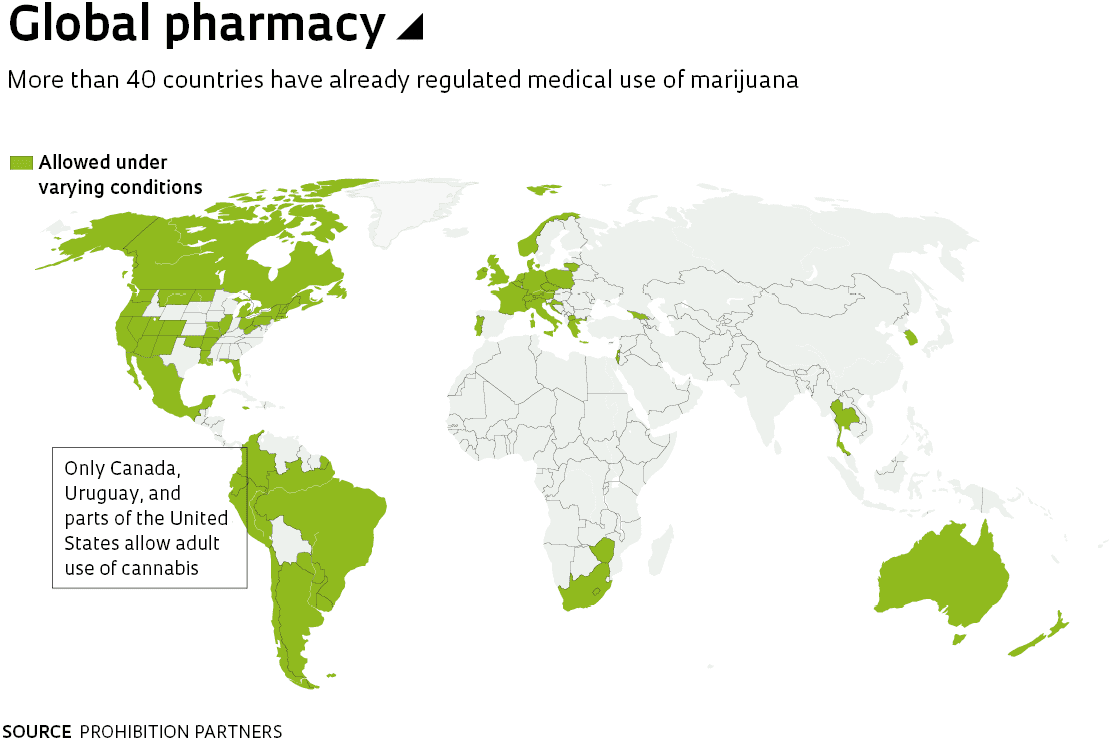
In addition to being a focus for research, its potential for contributing to a variety of treatments has made cannabis an increasingly frequent media topic in recent years. In parts of the United States and other countries such as Uruguay and Canada, measures were adopted that permit marijuana to be used medically—sometimes by smoking the herb itself—which has been a controversial decision.
In Brazil, this option is nowhere on the horizon. What has been proposed is the use of cannabidiol, the cannabinoid substance singled out as having therapeutic effects. “Actions like the Global Marijuana March have little effect,” says Antonio Zuardi. “The industry has realized that there’s a market, and that pressure is much stronger.” In December the Brazilian Health Regulatory Agency (ANVISA) approved a resolution that went into effect in March, allowing drugs with a predominance of cannabidiol as an active ingredient to be manufactured in Brazil. There are two categories, depending on the content of tetrahydrocannabidiol (THC) in the product’s composition (up to 0.2%, and more than 0.2%), and its sale in pharmacies (see timeline infographic). Products with a higher THC concentration may only be used with palliative care patients or those whose conditions are refractory to other medications or lower doses. Because THC is the substance responsible for the consciousness-altering, psychotropic effects of marijuana it is considered more dangerous. Authorizations will continue to be granted—as is the current practice—for compassionate use, i.e., when there are no effective medications available. The official denomination “cannabis-based products” means that these products would not yet be considered medicines, but the change would allow the pharmaceutical industry to make new products available in pharmacies on a provisional basis.
There were more than 6,000 applications for authorization to import cannabis-based drugs during the first quarter of 2019 alone. This market is expected to grow rapidly if domestic production is approved, although these compounds are not the cure-all solution commercial propaganda would like to suggest. Only one cannabis-based medicine is currently sold in Brazil, which interestingly enough has THC content equal to its CBD content. Mevatyl, authorized by ANVISA in 2017 for the control of spasms caused by multiple sclerosis, is produced by GW Pharmaceuticals, a leader in the international market based in England. Although its price has decreased, the cost of treatment is still high, around R$1,500 per 30 milliliters, an amount that lasts about a month depending on the case. The same drug is authorized in 28 countries, which do not include the United States, under the name Sativex.
Zuardi estimates that the first Brazilian pharmaceuticals to reach the market will be anticonvulsants for use in conjunction with other drugs in epileptic syndromes resistant to medication. “Optimistically, maybe even this year,” he predicts.
ABRACE, in Paraíba, is the only association with authorization to cultivate marijuana for patientsCésar Matos / ABRACE
Into the clinic The Ribeirão Preto group is at the forefront of research that may lead to the development of a new medicine that uses cannabidiol as its active ingredient, and has just concluded a clinical trial involving 15 children and adolescents between 2 and 18 years old, with a range of epileptic syndromes. The data are still under analysis, but Zuardi notes: “The results were excellent.” According to the researcher, in 60% of the patients the crises were cut by at least half, and 40% of that group were completely free of seizures. The reduction in crises was lower in the other 40% of patients, but one of the children saw no improvement.
It’s not enough, the psychiatrist admits. It was an open study, in which everyone knew the children were receiving the treatment. “Cannabidiol is famous, and just knowing they’re receiving this medication makes the families do the whole treatment more carefully,” he says. Reliable results are obtained only through double-blind trials, in which neither the patients’ families nor the researchers know which patients are medicated and which are receiving an innocuous substance, the placebo. “This study is ongoing, we’ve collected half of the data and we should be finished by mid-year,” he predicts.
Faced with the difficulty of obtaining the needed pharmacological agent in sufficient quantities for their tests, the Ribeirão Preto group signed an agreement with Prati-Donaduzzi pharmaceuticals, which is interested in developing drugs for this market. The test that was just completed was initially proposed in 2014, the same year that the GW lab registered a study for the same purpose on the clinicaltrials.gov website, which is the official international repository for such trials. The company made progress in testing and launched its antiepileptic drug Epidiolex in 2018, becoming the first medicine whose active ingredient is almost exclusively cannabidiol to be approved for sale in the United States. The Brazilian trial only began in 2018, when it received authorization from ANVISA. If it works, the drug produced will almost exclusively use CBD as its active ingredient, but dissolved in different excipients than its British counterpart.
Two-way street Brazilian studies in the field have a long history. In 1990, Guimarães, who had finished his doctorate a few years earlier under Zuardi’s guidance, published an article in the journal Psychopharmacology describing the results of a CBD study using the elevated plus maze—an anxiety-modeling test—with lab mice. The experiment showed that cannabidiol was an effective anxiolytic on test animals, but only in medium doses. When tested at higher doses the effect was lost, which would explain previous results from other groups that showed CBD was not suitable for treating anxiety.
As a consequence of his study, in 1991 Guimarães received a letter from Bulgarian-Israeli biochemist Raphael Mechoulam from Hebrew University of Jerusalem in Israel, who had been the first scientist to elucidate the chemical structures of CBD and THC, and was considered an authority on the subject. He proposed that Guimarães test the effects of changes to the molecular structure of CBD. The results, published in 1994 in the journal General Pharmacology, showed that certain modified forms of CBD (signified with the prefix HU, from “Hebrew University”) were as effective as natural cannabidiol in mice exploring the plus maze. Artificially altered molecules do not usually work well. These results, and others that followed, strengthened the collaborative relationship between Mechoulam’s group and the USP-RP group. One more recent result is the development and testing of modified CBD compounds with the addition of fluorine at different positions of the molecule. The superior efficacy of one of them—when compared to natural CBD—earned the Israeli and Brazilian groups a patent that was recently acquired by the American pharmaceuticals company Phytecs, which plans to develop dermatological medicines.
The Zuardi and Guimarães groups work in close collaboration within the scope of the National Science and Technology Institute for Translational Medicine (INCT-TM), coordinated by Jaime Hallak and José Alexandre Crippa. Translational medicine aims to use experiments carried out on animals to guide clinical trials, then work back toward animal models to thoroughly investigate the mechanisms behind observations made in patients, creating a two-way avenue of research. “The transposition between model and human being isn’t direct, but it provides important information for clinical studies, such as the pathways and safety of the drug,” says Zuardi. “If the drug shows a consistent effect without harm to the animals, we consider testing it on humans.”
Because of the way the endocannabinoid system functions (see infographic), he is emphatic regarding the potential for important medicines to come out of these studies. The psychiatrist explains that the brain has more receptors for cannabinoids than for the neurotransmitters that are recognized as central to its functioning. Every region of the nervous system is brimming with these receptors, which play a modulatory role. “If this is such an important system, drugs that interfere with it could also cause disease as much as they mitigate it,” says Zuardi. “Cannabidiol is like a Disneyland for pharmacologists,” jokes Guimarães. “More than 60 targets have already been described in studies done in vitro, but it’s not yet clear how the molecule acts in these receptors.” More than 100 cannabinoids are already known to exist in the Cannabis sativa plant, although with the overwhelming majority it’s still unclear as to their effects and actions on endocannabinoid receptors in animals.
Neuropsychiatric effect According to Guimarães, the large number of pharmacological targets with which CBD interacts to produce its effects contradicts a dogma in pharmacology, which states that the more specific a pharmaceutical is the better, because this minimizes the risk of adverse effects. The naturally systemic activity of cannabinoids, on the contrary, is at the heart of their pharmacological potential, and their low incidence of adverse effects. Serotonin, for example, an important neurotransmitter, is in some way modulated by cannabidiol, as shown by in vitro studies. Thus, any imbalance in this interaction can cause depression.
Indeed, evaluating the potential of cannabidiol as an antidepressant is a primary focus for the research group, as shown in an article led by pharmacologist Sâmia Joca, from the School of Pharmaceutical Sciences at USP-RP, published in February 2019 in the journal Molecular Neurobiology. The experiments subjected mice to forced-swim tests for five minutes, a common model for assessing the effect of antidepressants. The natural behavior of mice is to learn to float, making only the minimum movements necessary to keep their heads out of the water. When medicated with antidepressants, rodents swim more constantly, an effect that was also seen in cannabidiol tests. Injecting the compound into the abdominal cavity half an hour before the experiment gives the medication enough time to act, an effect that continues for up to seven days. The development of fast-acting antidepressants would be great news for those who sometimes need to wait weeks—with a risk of suicide in the most severe cases—until standard antidepressants begin to work.
The generalized action of CBD is also linked to its anti-inflammatory and antioxidant effects. “Inflammatory processes are behind many conditions linked to the central nervous system,” Guimarães observes. This could explain, among other effects, CBD’s neuroprotective role.
“We have strong indications that cannabinoids are beneficial for neurodegenerative diseases,” adds biomedical researcher Fernanda Crunfli, currently doing a postdoctoral internship at the Neuroproteomics Laboratory at the University of Campinas (UNICAMP), coordinated by biologist Daniel Martins-de-Souza. During her doctorate, supervised by biologist Andréa Torrão at USP’s Institute of Biomedical Sciences (ICB), she injected the brains of mice with streptozotocin, a compound that is toxic to the nervous system and capable of mimicking the neuronal death and cognitive impairment caused by Alzheimer’s disease. Rodents’ natural behavior is to investigate new objects longer than those already known to them, but this difference disappears when there is cognitive damage. Crunfli treated the test animals for seven days with the synthetic cannabinoid ACEA and saw that the mice began to have better memory function for recognizing objects. In addition, she verified that more cells survived due to an increase in production of the proteins that fight neuronal death caused by apoptosis, as shown in an article published in April in the journal Neurotoxicity Research. According to the researcher, this is because the drug reduces neuroinflammation and cell stress, which characterize neurodegenerative diseases such as Alzheimer’s.
Another characteristic effect of neurodegenerative diseases is a change in glucose metabolism, the source of energy in the nervous system. Crunfli is now studying this effect in the brains of mice through a collaborative study with physiologist Caroline Real, a postdoctoral researcher with the Hospital das Clínicas (HC) at the USP School of Medicine. Real is part of a research group headed by nuclear physician Carlos Buchpiguel and pharmaceutics researcher Daniele de Paula Faria. In preliminary results the group saw that treatment with either ACEA or CBD reversed cognitive impairments and improved glucose metabolism, giving the scientists a deeper understanding of the mechanisms involved.
There is evidence that people with schizophrenia may also benefit from cannabidiol, as Zuardi’s group showed with some of their first studies on patients, close to 25 years ago. It’s a tricky subject, partly because the risk of developing the disease triples for teenagers who have smoked large amounts of marijuana. When analyzed separately, it’s already known that THC worsens psychosis symptoms in schizophrenics.
CBD, on the other hand, appears to help control psychotic episodes. Various research groups are working to examine its effects in detail and transform this long history of study into proposals for treatment. “Some symptoms of schizophrenia, such as delusions and hallucinations, improve with existing antipsychotics,” says biomedical researcher Vanessa Abilio, from the Department of Pharmacology at the Federal University of São Paulo (UNIFESP). “Other symptoms like cognitive deficits, difficulty with social competence, and blunted affect, need new medication options.” Cannabidiol has emerged as a possible solution for these latter symptoms, which the group she coordinates is studying in animal models. Mice that have been induced to mimic the disease walk repetitively from side to side, a behavior that Abilio explains has a neurochemical basis similar to that of human delirium. They also show no particular interest in other mice that they encounter for the first time, a sign of social limitations.
The idea is to design a treatment using cannabidiol that can act as a preventative for people considered to be at high risk for developing schizophrenia due to family history or symptomatic changes in behavior. She and her colleagues explain their findings in an article published in the journal Frontiers in Pharmacology in 2018. However, there is still a long way to go from studies on animal models to a potential medication.
Biologist Renato Malcher of the University of Brasília (UnB) is also working on the frontier between studies in animal models and clinical approaches, and has confirmed a relationship exists, in rodents, between the endocannabinoid system and the probability of young being born with markers identified with autism. He was able to extend the study to humans thanks to AMA+ME, an association that provides Cannabis-based medication to patients who obtain judicial authorization. In 2016 they treated 18 autistic patients with a compound of CBD and THC—at a 75 to 1 ratio—for six to nine months. Malcher analyzed the results and detected improvements in a number of parameters, especially seizures, attention deficit disorder, sleep disorders, and difficulties in communication and social interaction in 14 of the patients (three abandoned the treatment and one did not respond to it), according to an article published in October 2019 in the journal Frontiers in Neurology. The caveat is that it was not a designed study, with all the controls necessary for a clinical trial. “It was the study that was possible: a number of patients requested treatment at the same time and the opportunity arose,” he says. Thus, the children’s improvement was measured according to their parents’ perceptions using standardized monthly questionnaires, and follow-up with the supervising clinician, Paulo Fleury-Teixeira. Similar results were reported by pediatrician Matitiahu Berkovitch’s group at the Assaf Harofeh Medical Center in Tel Aviv, Israel, published in January 2019 in the journal Frontiers in Pharmacology. Two months monitoring 53 children taking cannabidiol revealed improvements in a group of symptoms associated with autism, such as rage attacks, hyperactivity, sleep disorders, and anxiety, as reported by their parents.
Obstacle course Neuroscientist Renato Filev, a postdoctoral researcher in psychiatrist Dartiu Xavier da Silveira’s research group at the Federal University of São Paulo (UNIFESP), encountered challenges that are symptomatic of the way legislation acts as an obstacle to research on cannabinoids. During his doctoral research—under the guidance of neuroscientist Luiz Eugênio Mello, also at UNIFESP—he studied how THC acts against the effects of alcohol in mice, and published his findings in 2017 in the journal Alcohol. “The effect was satisfactory in reducing alcohol-induced locomotor activity,” he explains. Now, Filev wants to continue investigating the use of cannabinoids for the treatment of chemical addiction, specifically crack, continuing a study done by Silveira in the 1990s. But he still hasn’t been able to get the project under way.
In 2017 Filev obtained financing through an agreement between the National Drug Policy Secretariat (SENAD) and UNIFESP. But because protocols for obtaining a controlled substance—even through a corporate donation agreement—are not common at the university, bureaucratic procedures have not been established and ended up preventing the project from being executed. He is now looking for new funding and partnerships that will allow him to conduct clinical trials, which he argues would be innovative. “A gold standard for treating crack addiction doesn’t exist.”
The prospects of improving legal opportunities for researchers to obtain cannabidiol are slim: in December, ANVISA denied a regulation allowing cultivation of Cannabis sativa. For the time being, only the Brazilian Association for Cannabis Hope (ABRACE), established in 2015 in Paraíba, can plant marijuana and produce extracts for its associated patients.
Strains used for medicinal extracts have known levels of cannabinoidsLéo Ramos Chaves
From the domestic pharmacy to the market Due to the high prices, maze of bureaucracy, delays in delivery, and uncertainty in cannabinoid potency of imported extracts, many Brazilian families organize themselves through associations like ABRACE, obtaining individual judicial authorizations for artisanal cultivation and production of Cannabis oils. Such is the case of banker Maria Aparecida “Cidinha” Carvalho, who discovered in 2014 that CBD could help her daughter Clárian, then 10 years old, who suffers from Dravet’s Syndrome. In addition to frequent and prolonged seizures, the disease affects muscle tone and the ability to perspire, among other problems, making normal life impossible. Today Cidinha is president of Associação Cultive [Cultivate Association], whose science director is psychopharmacologist Elisaldo Carlini, of UNIFESP, a pioneer in the study of cannabinoids in Brazil. Through the association, the team teaches families how to obtain medication and how to extract oil from the plant.
Those who need cannabis-based drugs currently have several other challenges beyond cost, starting with finding a doctor willing to prescribe it. That’s why Viviane Sedola, who has a degree in public relations, founded Dr. Cannabis. The company maintains a platform that lists doctors who prescribe cannabinoids, which can be searched by patients. It also helps with preparing the documentation required to request ANVISA approval and aids in finding import suppliers for importation. In view of ANVISA’s recently announced changes that aim to reduce bureaucracy and speed up the process, Dr. Cannabis may have to shift its focus.
Sedola doesn’t see this as a problem: she’s been fighting for cannabinoids regulation, and notes that Canada is the only large country that has managed to regulate cannabis cultivation. “You can’t think only about agribusiness, only about the patient, only about the economy.” Because every side of the issue must be taken into consideration, she argues that the decision should come from legislative authorities, and says that a committee in the Brazilian House of Representatives has already taken action. In February, with former ANVISA president William Dib as a guest, the representatives met and went to Colombia to gain an understanding of the regulations there.
“I assume that cannabidiol, THC, and other cannabinoids will become official drugs and will be prescribed as such by doctors,” says Hebrew University researcher Mechoulam, who estimates that in Israel about 50,000 patients have authorized access to medical cannabis, for a variety of diseases. Cannabidiol is seen as safe because there is no record of deaths induced by its consumption, which doesn’t mean that it’s harmless. Its main problem seems to be that it inhibits liver enzymes that metabolize other drugs, so care must be taken with drug interactions in treatments that require a combination of medications. “All medicines are hazardous,” says Guimarães. “Some are useful.” In his opinion, there is no doubt that cannabinoids are. “Its therapeutic use is a path of no return,” he predicts.
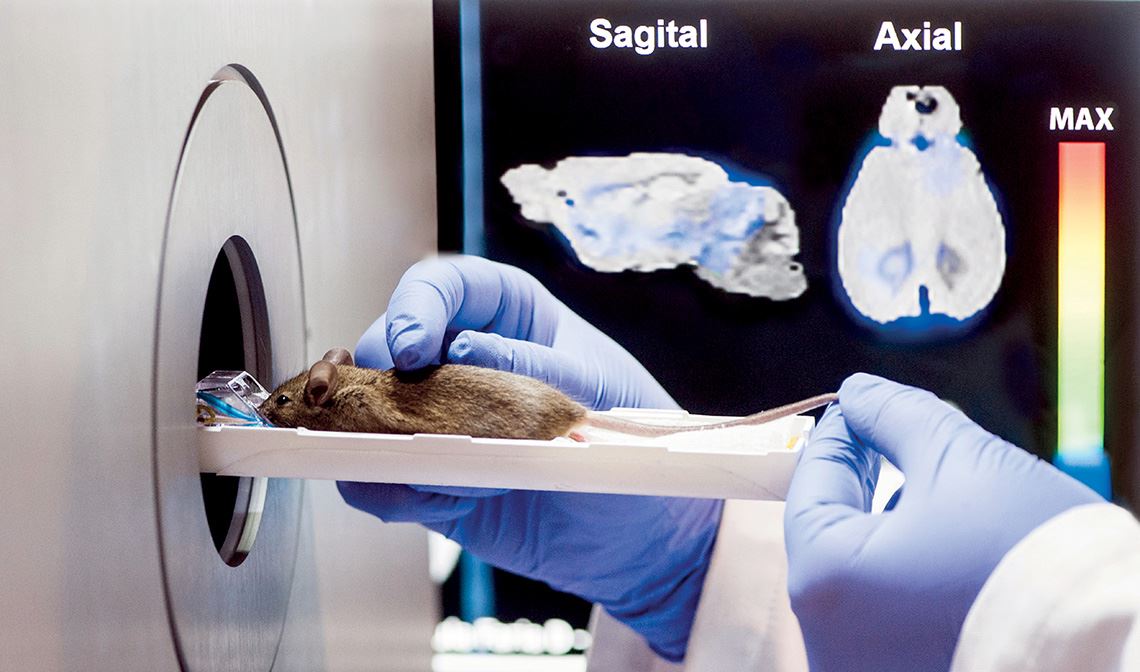
Mini-tomography for the brain Léo Ramos ChavesIn a pilot study, Caroline Real treated transgenic mice—which serve as a model for Alzheimer’s disease—with CBD provided by the Ribeirão Preto research group, as part of a collaboration between José Alexandre Crippa and psychiatrist Geraldo Busatto of FM-USP. The result was reduced neuroinflammation shown in positron emission tomography (PET) scans, and improvements in memory revealed by the object recognition test. “We’ve already seen progress in just 15 days of treatment,” she notes.
This article may be republished online under the CC-BY-NC-ND Creative Commons license. The Pesquisa FAPESP Digital Content Republishing Policy, specified here, must be followed. In summary, the text must not be edited and the author(s) and source (Pesquisa FAPESP) must be credited. Using the HTML button will ensure that these standards are followed. If reproducing only the text, please consult the Digital Republishing Policy.